

Embolization versus surgery for peptic ulcer bleeding after failed endoscopic hemostasis: a meta-analysis
- PMID: 26134614
- PMCID: PMC4423253
- DOI: 10.1055/s-0034-1365235
Embolization versus surgery for peptic ulcer bleeding after failed endoscopic hemostasis: a meta-analysis
Abstract
Background and study aims: A meta-analysis was conducted to assess the efficacy of transcatheter arterial embolization (TAE) compared with surgery in the management of patients with recurrent nonvariceal upper gastrointestinal bleeding (NVUGIB) after failure of endoscopic hemostasis.
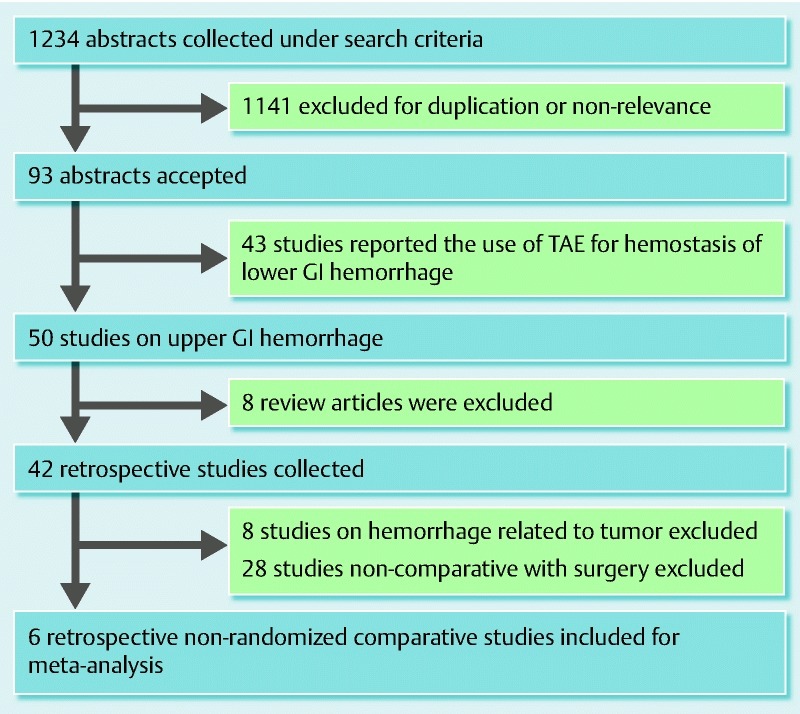
Patients and methods: Publications in English and non-English literatures (OVID, MEDLINE, and EMBASE) and abstracts from major international conferences were searched for studies comparing TAE with surgery for treatment of NVUGIB after endoscopic hemostasis failure. Outcome measures included rebleeding rate, all-cause mortality rate, and need for additional interventions to secure hemostasis.
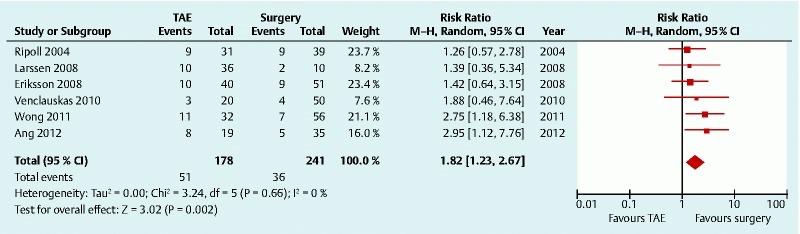
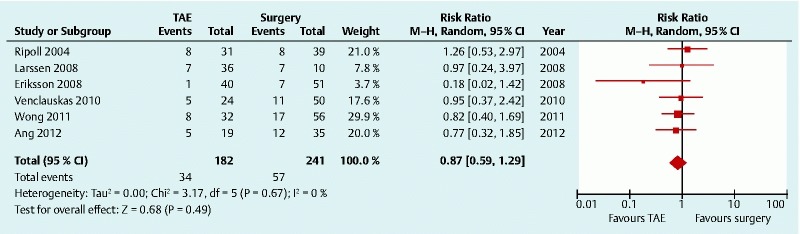
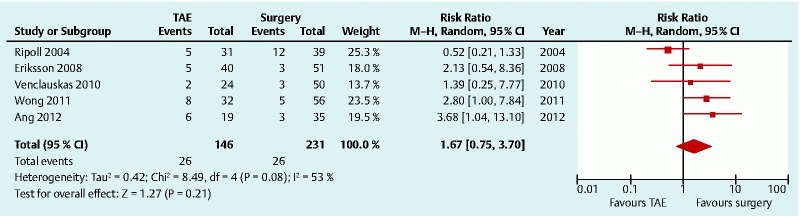
Results: From 1234 citations, 6 retrospective comparative studies were included that involved 423 patients (TAE, 182, 56 % male; surgery, 241, 68 % male). TAE patients were older (mean age, TAE 75, surgery, 68). The risk of rebleeding was significantly higher in TAE patients compared with surgically treated patients (relative risk [RR] 1.82, 95 % confidence interval [95 %CI] 1.23 - 2.67), with no statistically significant heterogeneity among the included studies (P = 0.66, I (2) = 0.0 %). After sensitivity analysis excluding studies with a large age difference between the two groups, a higher risk of bleeding remained in the TAE group (RR 2.64, 95 %CI] 1.48 - 4.71). No significant difference in mortality (RR 0.87, 95 %CI 0.59 - 1.29) or requirement for additional interventions (RR 1.67, 95 %CI 0.75 - 3.70) was shown between the two groups.
Conclusion: A higher rebleeding rate was observed after TAE, suggesting surgery more definitively secured hemostasis, with no significant difference in mortality rate or requirement of additional interventions. The TAE patients were older and in poorer health, thus future randomized studies are needed for accurate comparison of the two modalities.
Conflict of interest statement
Figures
References
-
- Cook D J, Guyatt G H, Salena B J. et al.Endoscopic therapy for acute nonvariceal upper gastrointestinal hemorrhage: a meta-analysis. Gastroenterology. 1992;102:139–148. - PubMed
-
- de Manzoni G Catalano F Festini M et al.Emorragia acuta da ulcera duodenale. Risultati del trattamento endoscopico del primo sanguinamento e delle recidive. (In Italian.) [Acute hemorrhage caused by duodenal ulcer. Results of endoscopic treatment of the first bleeding episode and of recurrences] Ann Ital Chir 200273387–394., discussion 394-396 - PubMed
-
- Cheynel N, Peschaud F, Hagry O. et al.Ulcère gastroduodénal hémorragique: résultats du traitement chirurgical. (in French). [Bleeding gastroduodenal ulcer: results of surgical management] Ann Chir. 2001;126:232–235. - PubMed
-
- Lau J Y, Sung J J, Lam Y H. et al.Endoscopic retreatment compared with surgery in patients with recurrent bleeding after initial endoscopic control of bleeding ulcers. N Engl J Med. 1999;340:751–756. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical