

Evaluation of feasibility, efficiency and safety of a pure NOTES gastrojejunal bypass with gastric outlet obstruction, in an in vivo porcine model
- PMID: 26135510
- PMCID: PMC4440371
- DOI: 10.1055/s-0033-1353686
Evaluation of feasibility, efficiency and safety of a pure NOTES gastrojejunal bypass with gastric outlet obstruction, in an in vivo porcine model
Abstract
Introduction: Natural orifice transluminal endoscopic surgery (NOTES) gastrojejunal anastomosis (GJA) is a less invasive surgery for bariatric procedures and gastric outlet obstruction. The aim of this study was to evaluate the feasibility, efficacy, and safety of a pure NOTES gastrojejunal bypass using an in vivo porcine model.
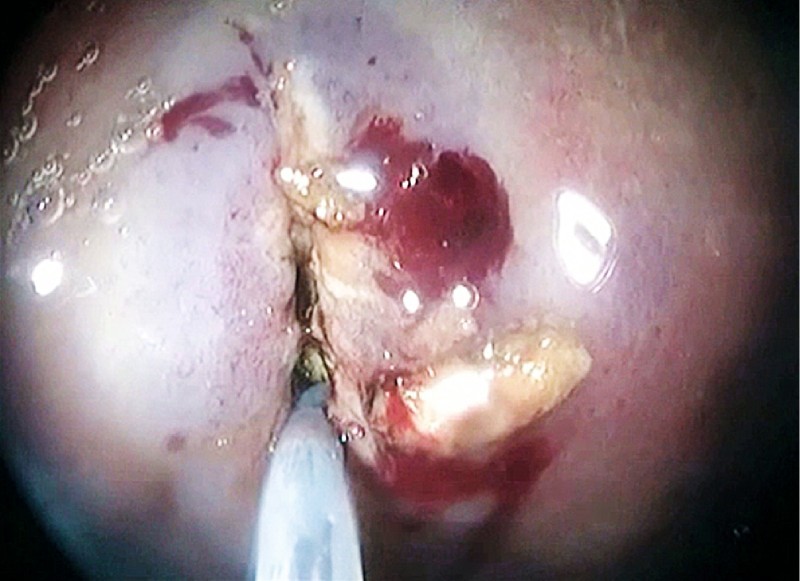
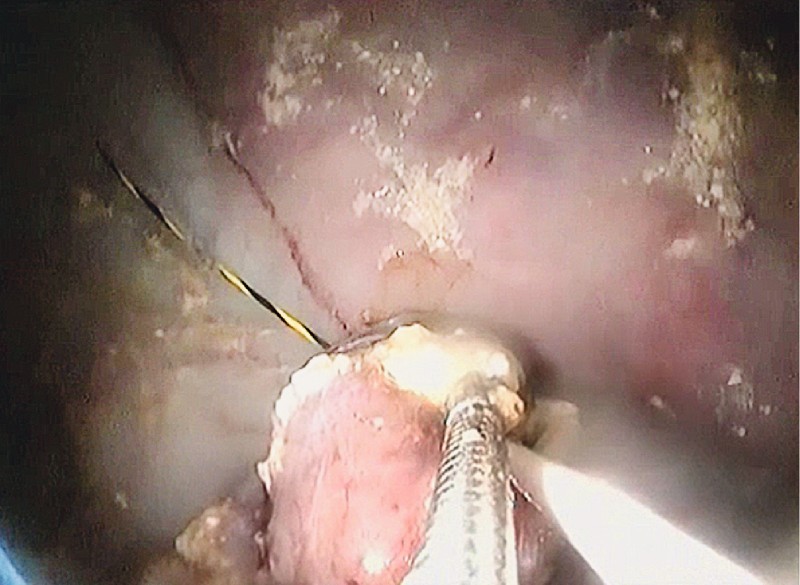
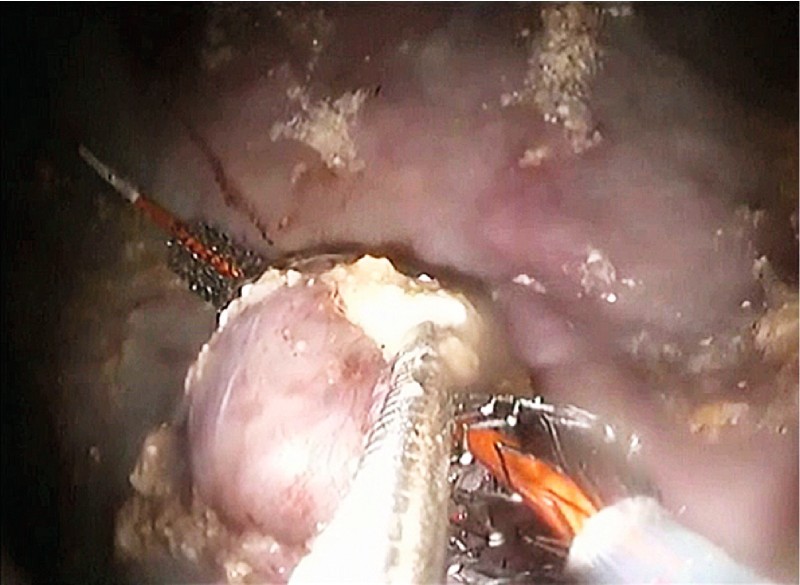
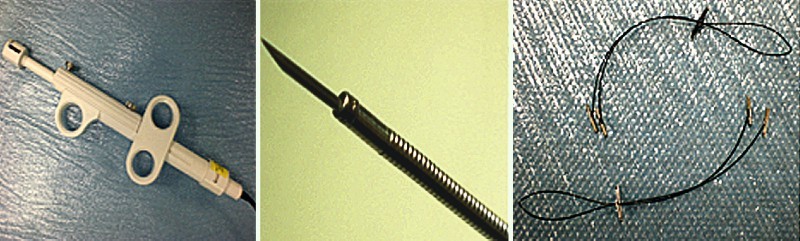
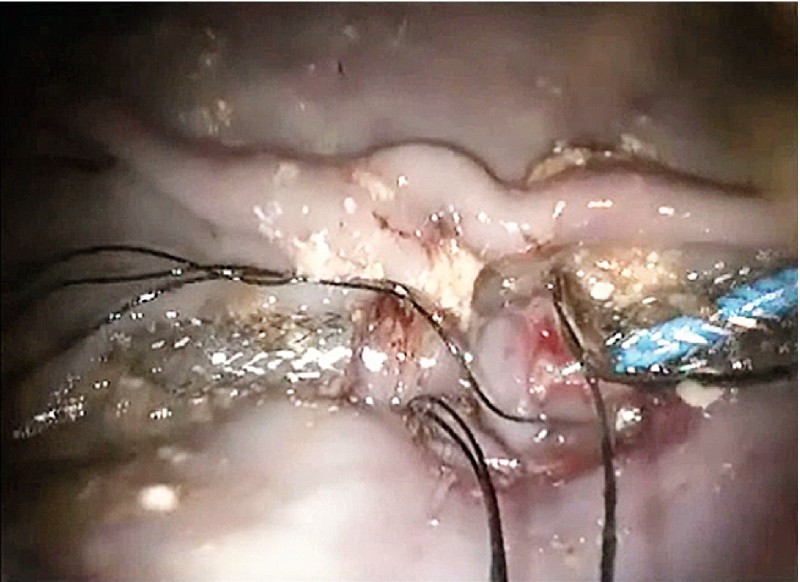
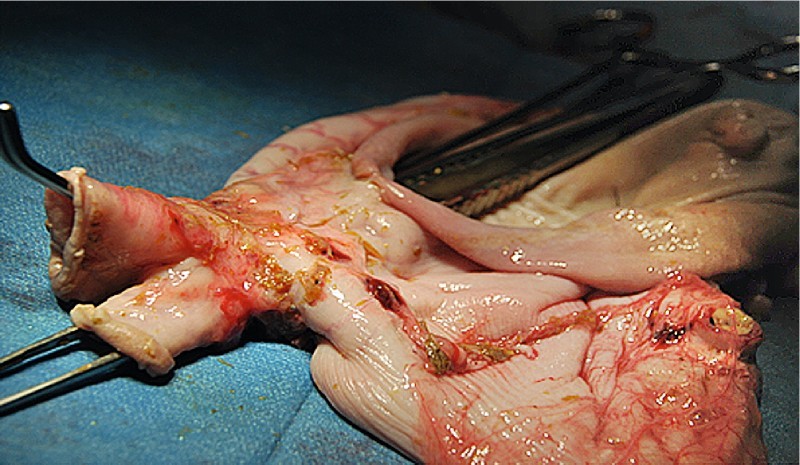
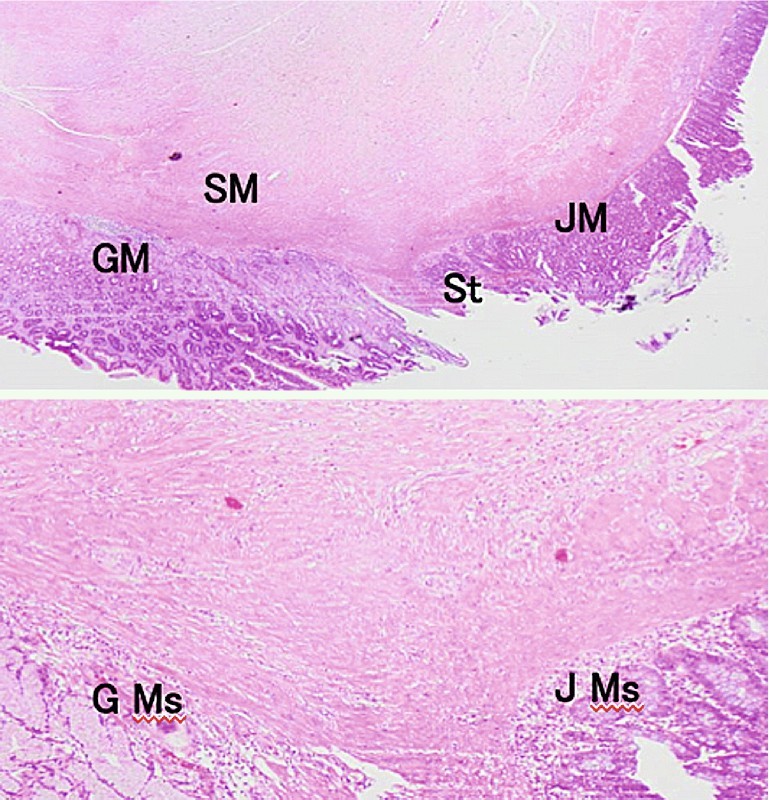
Material and methods: A prospective study was performed on nine swine. A double-channel scope was used. The intervention steps were: (i) gastric incision; (ii) peritoneal access; (iii) jejunal loop selection and mobilization into the stomach; (iv) stoma creation within the gastric wall and incision; (v) anastomosis suture and pylorus closure using a T-tag prototype. The animals were assessed clinically for 3 weeks including the weight gain. The patency of the GJA was assessed at necropsy and a histological analysis was performed.
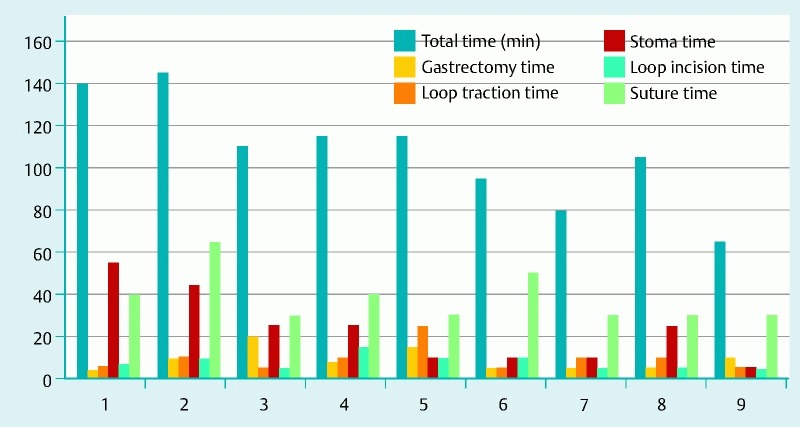
Results: We successfully performed all the procedures with a mean (standard deviation [SD]) operative time of 108 (26) minutes. We used a mean of 5.55 (1.30) stitches. There were no intraprocedural adverse events. Five animals survived up till euthanasia at 3 weeks (65 %). These showed a significant difference in weight curves of a loss of 3.2 kg compared with gain of 5.2 kg in a control group. Four pigs died from anastomotic dehiscence complicated by peritonitis.
Conclusion: Gastrojejunal bypass with a pure NOTES approach is feasible. This procedure is effective, resulting in a patent anastomosis and a significant weight loss. However, the anastomotic dehiscence is a major concern because of its mortality rate, and further studies including improvement of the suturing device and the technique are needed.
Conflict of interest statement
Figures

Similar articles
-
Gastrojejunal anastomosis using a tissue-apposing stent: a safety and feasibility study in live pigs.Endoscopy. 2014 Oct;46(10):871-7. doi: 10.1055/s-0034-1377347. Epub 2014 Jul 14. Endoscopy. 2014. PMID: 25019971
-
Gastrojejunal Anastomosis Exclusively Using the "NOTES" Technique in Live Pigs: A Feasibility and Reliability Study.Surg Innov. 2014 Aug;21(4):409-18. doi: 10.1177/1553350613508016. Epub 2013 Nov 19. Surg Innov. 2014. PMID: 24253256
-
Feasibility of Conversion of a New Bariatric Fully Endoscopic Bypass Procedure to Bariatric Surgery: a Porcine Pilot Study.Obes Surg. 2022 Jul;32(7):2280-2288. doi: 10.1007/s11695-022-06065-1. Epub 2022 Apr 25. Obes Surg. 2022. PMID: 35469079
-
Efficacy of endoscopic gastrojejunal bypass in obese Yucatan pigs: a comparative animal study.BMC Gastroenterol. 2023 Nov 1;23(1):375. doi: 10.1186/s12876-023-03000-1. BMC Gastroenterol. 2023. PMID: 37915010 Free PMC article.
-
Current applications of endoscopic suturing.World J Gastrointest Endosc. 2015 Jul 10;7(8):777-89. doi: 10.4253/wjge.v7.i8.777. World J Gastrointest Endosc. 2015. PMID: 26191342 Free PMC article. Review.
Cited by
-
First fully endoscopic metabolic procedure with NOTES gastrojejunostomy, controlled bypass length and duodenal exclusion: a 9-month porcine study.Sci Rep. 2022 Jan 7;12(1):21. doi: 10.1038/s41598-021-02921-9. Sci Rep. 2022. PMID: 34996894 Free PMC article.
-
Endoscopic esophagogastric anastomosis with luminal apposition Axios stent (LAS) approach: a new concept for hybrid "Lewis Santy".Endosc Int Open. 2017 Jun;5(6):E455-E462. doi: 10.1055/s-0043-106577. Epub 2017 May 31. Endosc Int Open. 2017. PMID: 28573178 Free PMC article.
References
-
- Dray X, Marteau P. [The future of gastrointestinal therapeutic endoscopy: NOTES] Gastroenterol Clin Biol. 2009;33:758–766. - PubMed
-
- Giday S A, Kantsevoy S V, Kalloo A N. Principle and history of Natural Orifice Translumenal Endoscopic Surgery (NOTES) Minim Invasive Ther Allied Technol. 2006;15:373–377. - PubMed
-
- Ly J, O’Grady G, Mittal A. et al.A systematic review of methods to palliate malignant gastric outlet obstruction. Surg Endosc. 2010;24:290–297. - PubMed
-
- Jeurnink S M, Steyerberg E W, van Hooft J E. et al.Surgical gastrojejunostomy or endoscopic stent placement for the palliation of malignant gastric outlet obstruction (SUSTENT study): a multicenter randomized trial. Gastrointest Endosc. 2010;71:490–499. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources