

Therapeutic efficacy of umbilical cord-derived mesenchymal stem cells in patients with type 2 diabetes
- PMID: 26136869
- PMCID: PMC4471780
- DOI: 10.3892/etm.2015.2339
Therapeutic efficacy of umbilical cord-derived mesenchymal stem cells in patients with type 2 diabetes
Abstract
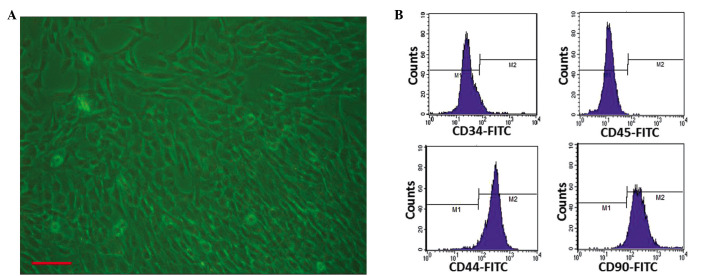
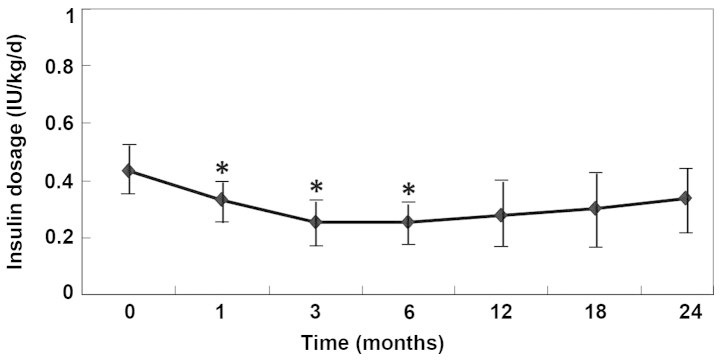
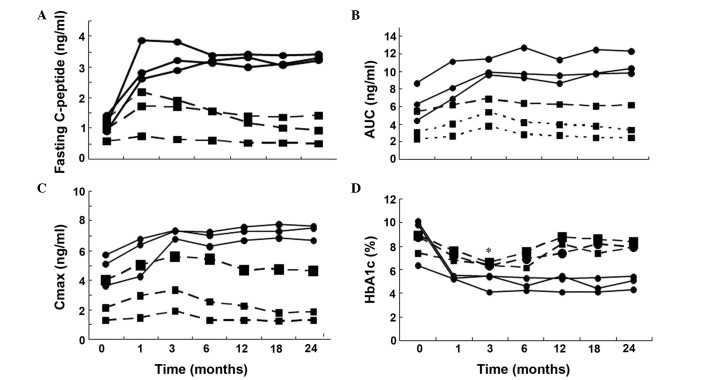
Type 2 diabetes (T2D) is characterized by progressive and inexorable β-cell dysfunction, leading to insulin deficiency. Novel strategies to preserve the remaining β-cells and restore β-cell function for the treatment of diabetes are urgently required. Mesenchymal stem cells (MSCs) have been exploited in a variety of clinical trials aimed at reducing the burden of immune-mediated disease. The aim of the present clinical trial was to assess the safety and efficacy of umbilical cord-derived MSC (UCMSC) transplantation for patients with T2D. The safety and efficacy of UCMSC application were evaluated in six patients with T2D during a minimum of a 24-month follow-up period. Following transplantation, the levels of fasting C-peptide, the peak value and the area under the C-peptide release curve increased significantly within one month and remained high during the follow-up period (P<0.05). Three of the six patients became insulin free for varying lengths of time between 25 and 43 months, while the additional three patients continued to require insulin injections, although with a reduced insulin requirement. Fasting plasma glucose and 2-h postprandial blood glucose levels were relatively stable in all the patients following transplantation. There was no immediate or delayed toxicity associated with the cell administration within the follow-up period. Therefore, the results indicated that transplantation of allogeneic UCMSCs may be an approach to improve islet function in patients with T2D. There were no safety issues observed during infusion and the long-term monitoring period.
Keywords: cytotherapy; diabetes; mesenchymal stem cells.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical