

Tumor size and lymph node status determined by imaging are reliable factors for predicting advanced cervical cancer prognosis
- PMID: 26137044
- PMCID: PMC4467330
- DOI: 10.3892/ol.2015.3015
Tumor size and lymph node status determined by imaging are reliable factors for predicting advanced cervical cancer prognosis
Abstract
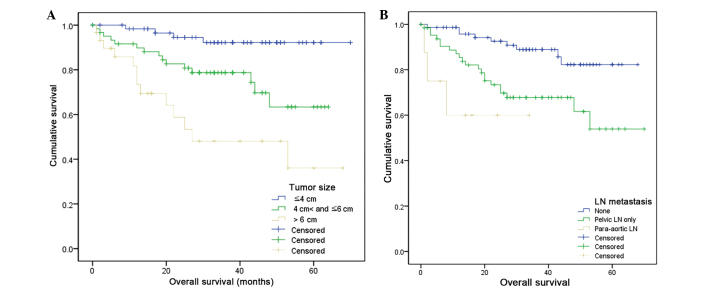
The aim of the present study was to investigate the prognostic role of a number of clinical factors in advanced cervical cancer patients. Patients (n=157) with stage IIA-IIB cervical cancer treated at four Hallym Medical Centers in South Korea (Hallym University Sacred Heart Hospital; Kangnam Sacred Heart Hospital; Chuncheon Sacred Heart Hospital; and Kangdong Sacred Heart Hospital) between 2006 and 2010 were retrospectively enrolled. Univariate analysis identified significant predictive values in the following eight factors: i) Cancer stage (P<0.0001); ii) tumor size (≤4 vs. 4-6 cm, P=0.0147; and ≤4 vs. >6 cm, P<0.0001); iii) serum squamous cell carcinoma antigen level (≤2 vs. >15 ng/ml; P=0.0291); iv) lower third vaginal involvement (P<0.0001); v) hydronephrosis (P=0.0003); vi) bladder/rectum involvement (P=0.0015); vii) pelvic (P=0.0017) or para-aortic (P=0.0019) lymph node (LN) metastasis detected by imaging vs. no metastasis; and viii) pelvic LN metastasis identified by pathological analysis (P=0.0289). Furthermore, multivariate analysis determined that tumor size (≤4 vs. 4-6 cm, P=0.0371; and ≤4 vs. >6 cm, P=0.0024) and pelvic LN metastasis determined by imaging vs. no metastasis (P=0.0499) were independent predictive variables. Therefore, tumor size and pelvic LN metastasis measured by imaging were independent predictive factors for the prognosis of advanced cervical cancer. These factors may provide more clinically significant prognostic information compared with the currently used International Federation of Gynecology and Obstetrics staging system.
Keywords: pelvic lymph node; prognosis; tumor size; uterine cervical cancer.
Figures

Similar articles
-
[Clinical significance of serum squamous cell carcinoma antigen in patients with early cervical squamous cell carcinoma].Zhonghua Zhong Liu Za Zhi. 2019 May 23;41(5):357-362. doi: 10.3760/cma.j.issn.0253-3766.2019.05.007. Zhonghua Zhong Liu Za Zhi. 2019. PMID: 31137169 Chinese.
-
[Long-term oncological outcomes after laparoscopic versus abdominal radical hysterectomy in stage I a2- II a2 cervical cancer: a matched cohort study].Zhonghua Fu Chan Ke Za Zhi. 2015 Dec;50(12):894-901. Zhonghua Fu Chan Ke Za Zhi. 2015. PMID: 26887872 Chinese.
-
Para-aortic lymph node involvement revisited in the light of the revised 2018 FIGO staging system for cervical cancer.Arch Gynecol Obstet. 2019 Sep;300(3):675-682. doi: 10.1007/s00404-019-05232-7. Epub 2019 Jul 1. Arch Gynecol Obstet. 2019. PMID: 31263988
-
[Outcomes and prognostic factors of distant metastasis in patients with advanced cervical squamous cell carcinoma treated with concurrent chemoradiotherapy].Zhonghua Fu Chan Ke Za Zhi. 2015 Feb;50(2):125-30. Zhonghua Fu Chan Ke Za Zhi. 2015. PMID: 25877610 Chinese.
-
Standardized uptake value and metabolic tumor volume measured by ¹⁸F FDG PET/CT are sensitive biomarkers for the presence of lymph node metastasis in patients with cervical carcinoma.Rev Esp Med Nucl Imagen Mol. 2014 Sep-Oct;33(5):268-73. doi: 10.1016/j.remn.2013.05.007. Epub 2014 Jul 8. Rev Esp Med Nucl Imagen Mol. 2014. PMID: 25018135
Cited by
-
Usefulness of the maximum standardized uptake value for the diagnosis and staging of patients with cervical cancer undergoing positron emission tomography/computed tomography.Medicine (Baltimore). 2018 Feb;97(7):e9856. doi: 10.1097/MD.0000000000009856. Medicine (Baltimore). 2018. PMID: 29443749 Free PMC article.
-
Conditional relative survival of cervical cancer: a Korean National Cancer Registry Study.J Gynecol Oncol. 2021 Jan;32(1):e5. doi: 10.3802/jgo.2021.32.e5. Epub 2020 Oct 26. J Gynecol Oncol. 2021. PMID: 33185046 Free PMC article.
-
Radiological evaluation of metastatic lymph nodes in carcinoma cervix with emphasis on their infiltrative pattern.Indian J Med Res. 2021 Aug;154(2):383-390. doi: 10.4103/ijmr.IJMR_212_21. Indian J Med Res. 2021. PMID: 35295016 Free PMC article.
-
Survival outcomes of patients with cervical cancer and accompanying hydronephrosis: A systematic review of the literature.Oncol Rev. 2019 Jan 15;13(1):387. doi: 10.4081/oncol.2019.387. eCollection 2019 Jan 14. Oncol Rev. 2019. PMID: 30746036 Free PMC article.
-
Predictive Role of Preoperative Whole-Body 18F-FDG PET/CT for Risk Stratification of Early-Stage (FIGO I-IIA) Cervical Cancer Patients Treated by Surgery.Cureus. 2024 Jan 28;16(1):e53107. doi: 10.7759/cureus.53107. eCollection 2024 Jan. Cureus. 2024. PMID: 38283777 Free PMC article.
References
-
- Ferlay J, Soerjomataram I, Ervik M, et al., editors. GLOBOCAN 2008: Cancer incidence, mortality and prevalence worldwide. IARC Press; Lyon: 2008.
-
- Lilic V, Lilic G, Filipovic S, Milosevic J, Tasic M, Stojilijkovic M. Modern treatment of invasive carcinoma of the uterine cervix. J BUON. 2009;14:587–592. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources