

Baker's Cyst: Diagnostic and Surgical Considerations
- PMID: 26137182
- PMCID: PMC4481672
- DOI: 10.1177/1941738113520130
Baker's Cyst: Diagnostic and Surgical Considerations
Abstract
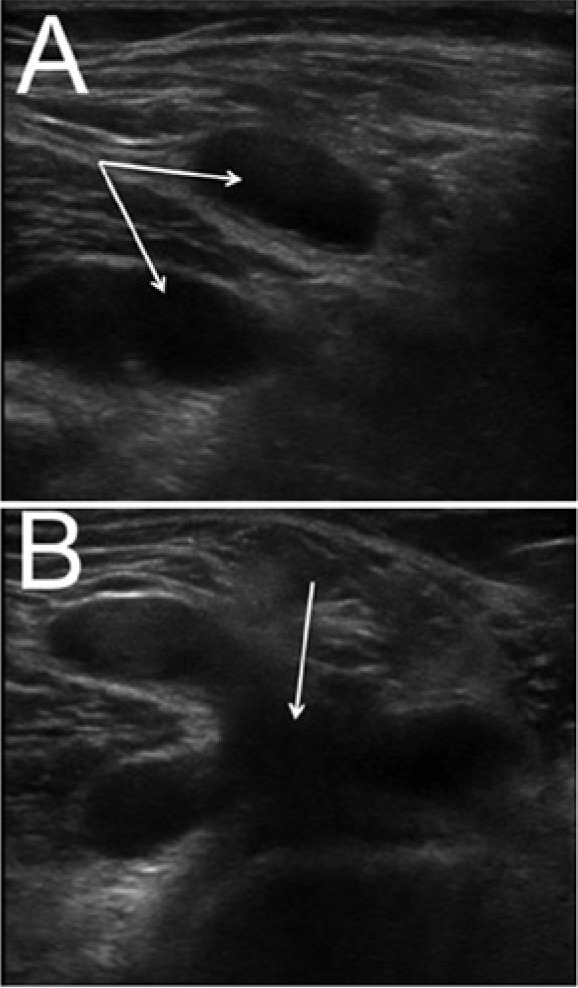
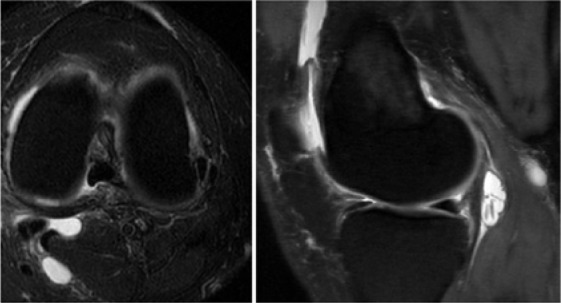
Context: Popliteal synovial cysts, also known as Baker's cysts, are commonly found in association with intra-articular knee disorders, such as osteoarthritis and meniscus tears. Histologically, the cyst walls resemble synovial tissue with fibrosis evident, and there may be chronic nonspecific inflammation present. Osteocartilaginous loose bodies may also be found within the cyst, even if they are not seen in the knee joint. Baker's cysts can be a source of posterior knee pain that persists despite surgical treatment of the intra-articular lesion, and they are routinely discovered on magnetic resonance imaging scans of the symptomatic knee. Symptoms related to a popliteal cyst origin are infrequent and may be related to size.
Evidence acquisition: A PubMed search was conducted with keywords related to the history, diagnosis, and treatment of Baker's cysts-namely, Baker's cyst, popliteal cyst, diagnosis, treatment, formation of popliteal cyst, surgical indications, and complications. Bibliographies from these references were also reviewed to identify related and pertinent literature.
Study design: Clinical review.
Level of evidence: Level 4.
Results: Baker's cysts are commonly found associated with intra-articular knee disorders. Proper diagnosis, examination, and treatment are paramount in alleviating the pain and discomfort associated with Baker's cysts.
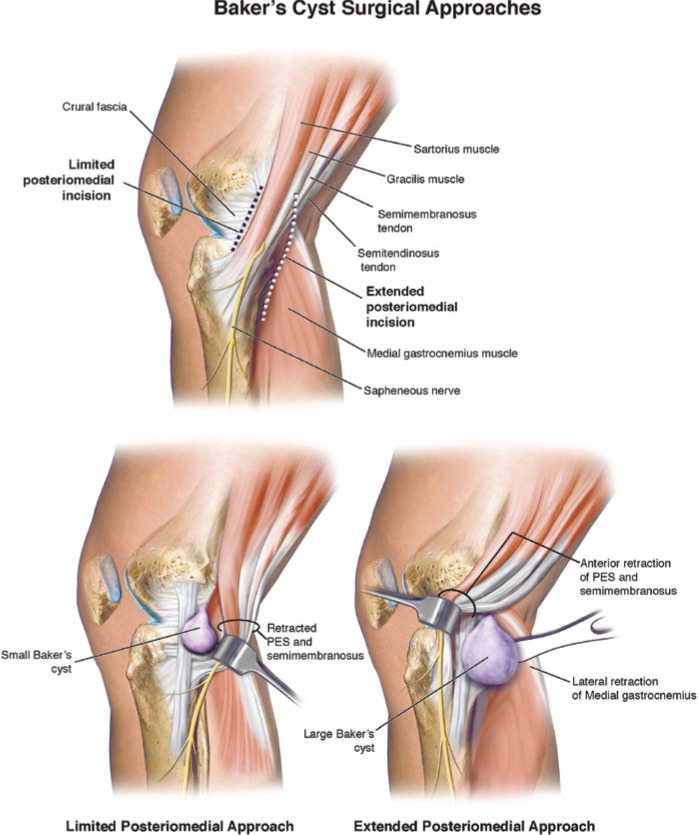
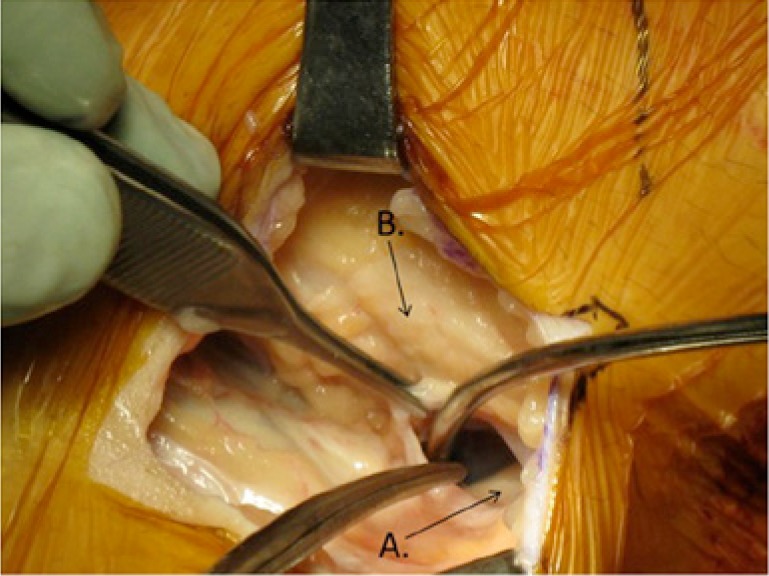
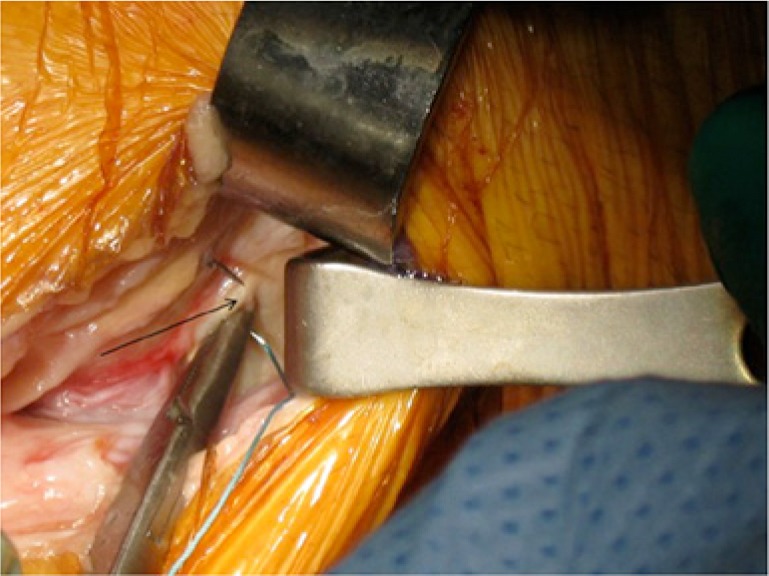
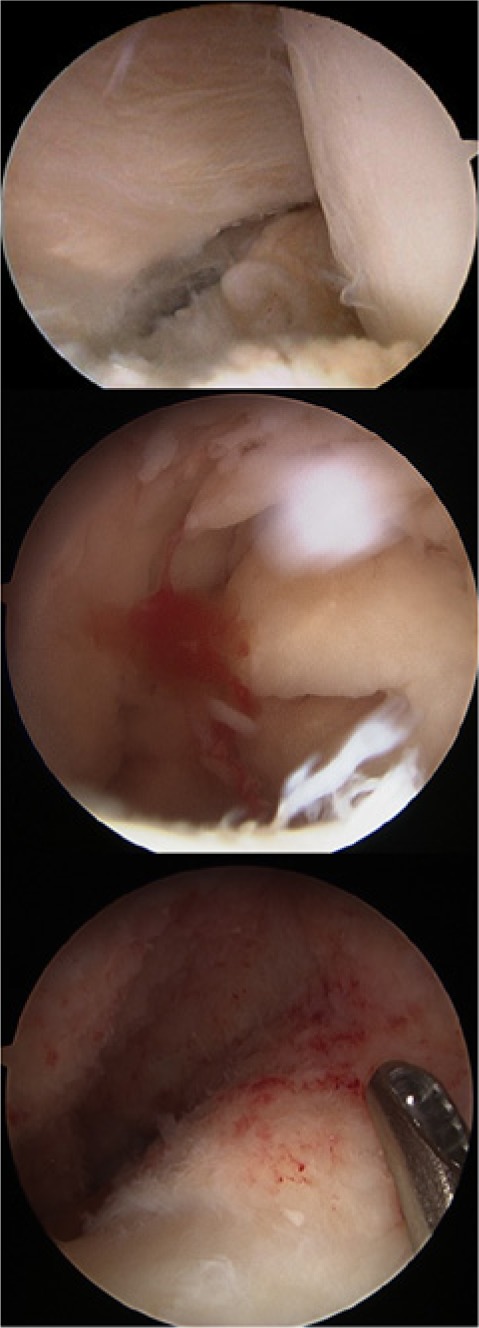
Conclusion: A capsular opening to the semimembranosus-medial head gastrocnemius bursa is a commonly found normal anatomic variant. It is thought that this can lead to the formation of a popliteal cyst in the presence of chronic knee effusions as a result of intra-articular pathology. Management of symptomatic popliteal cysts is conservative. The intra-articular pathology should be first addressed by arthroscopy. If surgical excision later becomes necessary, a limited posteromedial approach is often employed. Other treatments, such as arthroscopic debridement and closure of the valvular mechanism, are not well studied and cannot yet be recommended.
Keywords: Baker’s cysts; intra-articular knee disorders; popliteal synovial cysts.
Conflict of interest statement
The following author declared potential conflicts of interest: Frank R. Noyes, MD, receives fellowship support from DJO Global, Inc and Arthrex, Inc.
Figures

References
-
- Acebes JC, Sanchez-Pernaute O, Diaz-Oca A, Herrero-Beaumont G. Ultrasonographic assessment of Baker’s cysts after intra-articular corticosteroid injection in knee osteoarthritis. J Clin Ultrasound. 2006;34:113-117. - PubMed
-
- Adams R. Chronic rheumatic arthritis of the knee joint. Dublin J Med Sci. 1840;17:520-522.
-
- Baker WM. On the formation of synovial cysts in the leg in connection with disease of the knee joint. 1877. Clin Orthop Relat Res. 1994;299:2-10. - PubMed
-
- Bryan RS, DiMichele JD, Ford GL., Jr. Popliteal cysts. Arthrography as an aid to diagnosis and treatment. Clin Orthop Relat Res. 1967;50:203-208. - PubMed
-
- Calvisi V, Lupparelli S, Giuliani P. Arthroscopic all-inside suture of symptomatic Baker’s cysts: a technical option for surgical treatment in adults. Knee Surg Sports Traumatol Arthrosc. 2007;15:1452-1460. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
