

Extracranial metastasis of gliobastoma: Three illustrative cases and current review of the molecular pathology and management strategies
- PMID: 26137254
- PMCID: PMC4471516
- DOI: 10.3892/mco.2015.494
Extracranial metastasis of gliobastoma: Three illustrative cases and current review of the molecular pathology and management strategies
Abstract
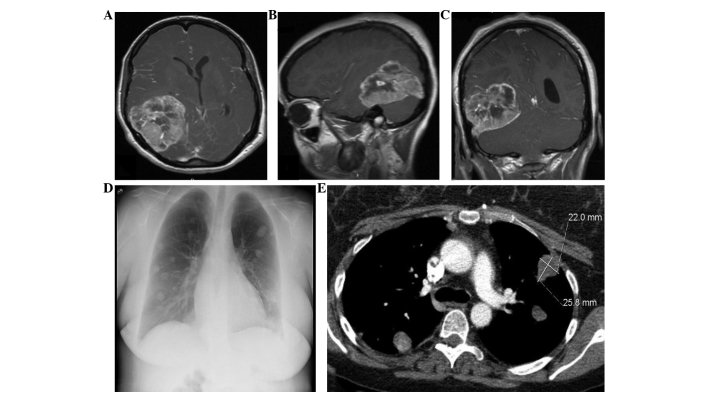
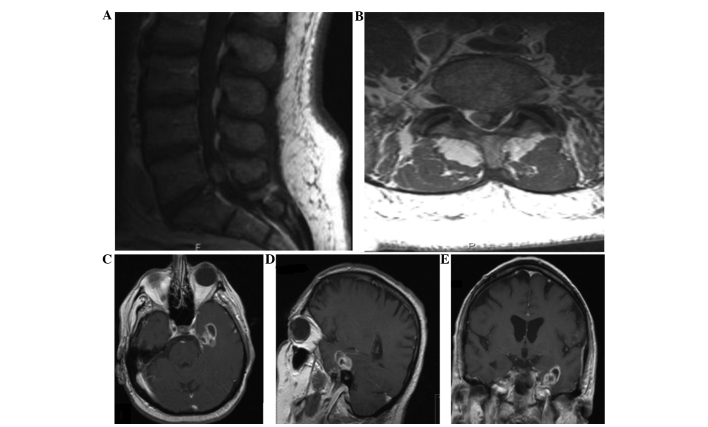
Glioblastoma (GBM) is the most common and the most malignant primary brain tumor in adults, accounting for ~12-15% of all intracranial neoplasms. Despite advances in surgical, medical and radiation therapies, the mortality of GBM remains high, with a median survival ranging between 40 and 70 weeks. Similar to other primary brain tumors, the extracranial metastasis of GBM is extremely rare, occurring in <2% of patients. To demonstrate the clinical characteristics of this rare tumor, we herein present three cases of extracranial GBM metastasis: One to the lungs, which represents the longest reported survival of lung metastases from GBM to date; the second to the soft tissue of the posterior neck; and the third to the lumbar intradural space. Unlike tumors elsewhere, there are unique barriers in the brain that prevent the hematogenous and lymphatic spread of intracranial tumors, such as the dura mater and the thickened basement membrane of the blood vessels. In addition, central nervous system tumor cells lack extracellular matrix proteins required to invade surrounding connective tissue, a prerequisite for tumor dissemination. In this study, we aimed to investigate the different possible mechanisms underlying the extracranial metastasis of GBM and determine the biomolecular and genetic characteristics differentiating GBMs that metastasize from those that do not. We also reviewed the role of systemic chemotherapy and bevacizumab in the treatment of disseminated GBMs. Early identification and differentiation of these tumors may enable patients to benefit from surgical resection, radiation and combination chemotherapy prior to developing other comorbidities from metastatic disease, which may translate into prolonged survival with an acceptable quality of life.
Keywords: bevacizumab; glial fibrillary acidic protein; glioblastoma; metastasis; temozolomide.
Figures

References
-
- Datta CK, Weinstein JD, Bland JE, Brager PM, Stewart MA. A case of cervical lymph node metastasis resulting from glioblastoma multiforme. W V Med J. 1998;94:276–278. - PubMed
-
- Fecteau AH, Penn I, Hanto DW. Peritoneal metastasis of intracranial glioblastoma via a ventriculoperitoneal shunt preventing organ retrieval: case report and review of the literature. Clin Transplant. 1998;12:348–350. - PubMed
-
- Piccirilli M, Brunetto GM, Rocchi G, Giangaspero F, Salvati M. Extra central nervous system metastases from cerebral glioblastoma multiforme in elderly patients. Clinico-pathological remarks on our series of seven cases and critical review of the literature. Tumori. 2008;94:40–51. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources