

Expression of Cathepsins B, D, and G in Infantile Hemangioma
- PMID: 26137466
- PMCID: PMC4470331
- DOI: 10.3389/fsurg.2015.00026
Expression of Cathepsins B, D, and G in Infantile Hemangioma
Abstract
Aims: The role of the renin-angiotensin system (RAS) in the biology of infantile hemangioma (IH) represents an emerging paradigm, particularly the involvement of renin, angiotensin converting enzyme, and angiotensin II. This study investigated the expression of cathepsins B, D, and G, enzymes that may modulate the RAS, in IH.
Materials and methods: The expression of cathepsins B, D, and G was examined using immunohistochemistry, enzyme activity assays, mass spectrometry, and NanoString gene expression assay in IH samples at different phases of development.
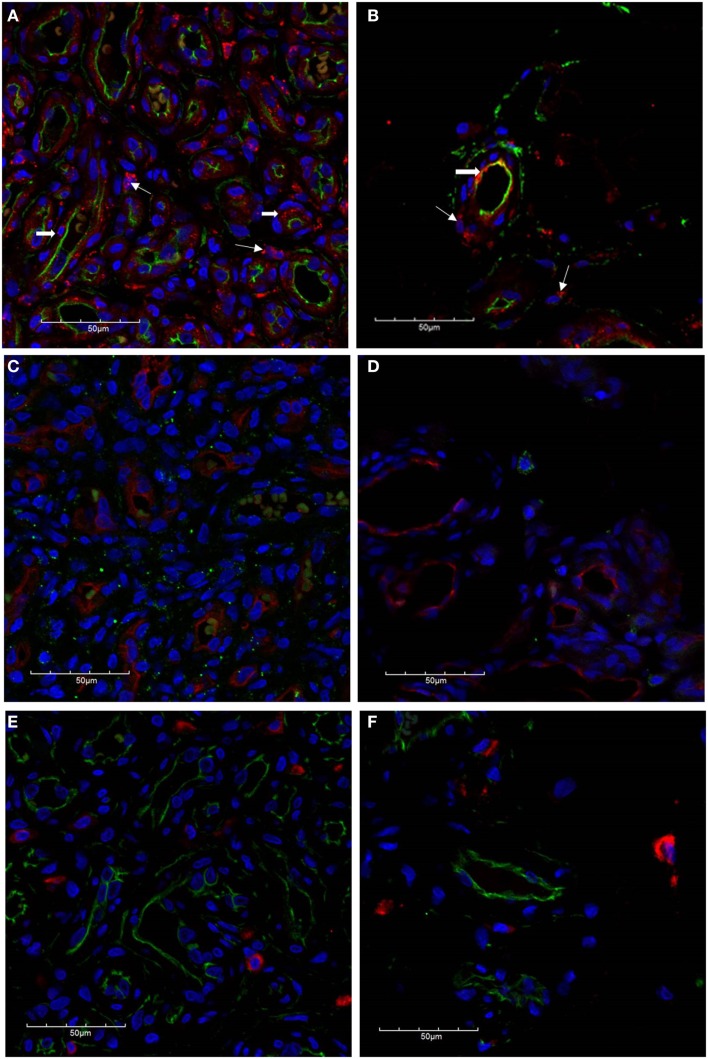
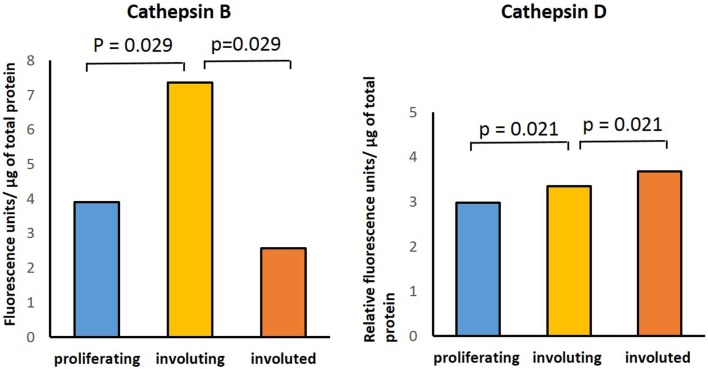
Results: Immunohistochemical staining showed the expression of cathepsins B, D, and G in proliferating and involuted IH samples. This was confirmed at the transcriptional level using NanoString gene expression assays. Mass spectrometry confirmed the identification of cathepsins D and G in all three phases of IH development, whereas cathepsin B was detected in 2/2 proliferating and 1/2 involuting lesions. Enzyme activity assays demonstrated the activity of cathepsins B and D, but not G, in all phases of IH development.
Conclusion: Our data demonstrated the presence of cathepsins B, D, and G in IH. Their role in modulating the RAS and the biology of IH offers potential novel targets for the management of this tumor.
Keywords: angiotensin converting enzyme; cathepsin; infantile hemangioma; paracrine; renin–angiotensin system.
Figures




Similar articles
-
Expression of Cathepsins B, D, and G in WHO Grade I Meningioma.Front Surg. 2019 Mar 12;6:6. doi: 10.3389/fsurg.2019.00006. eCollection 2019. Front Surg. 2019. PMID: 30949483 Free PMC article.
-
Expression of Cathepsins B, D, and G by the Embryonic Stem Cell-Like Population within Human Keloid Tissues and Keloid-Derived Primary Cell Lines.Plast Reconstr Surg. 2019 Dec;144(6):1338-1349. doi: 10.1097/PRS.0000000000006275. Plast Reconstr Surg. 2019. PMID: 31764649
-
Expression and Localization of Cathepsins B, D, and G in Dupuytren's Disease.Plast Reconstr Surg Glob Open. 2018 Feb 14;6(2):e1686. doi: 10.1097/GOX.0000000000001686. eCollection 2018 Feb. Plast Reconstr Surg Glob Open. 2018. PMID: 29616179 Free PMC article.
-
Biology of infantile hemangioma.Front Surg. 2014 Sep 25;1:38. doi: 10.3389/fsurg.2014.00038. eCollection 2014. Front Surg. 2014. PMID: 25593962 Free PMC article. Review.
-
Cardiovascular drugs in the treatment of infantile hemangioma.World J Cardiol. 2016 Jan 26;8(1):74-80. doi: 10.4330/wjc.v8.i1.74. World J Cardiol. 2016. PMID: 26839658 Free PMC article. Review.
Cited by
-
Propranolol in the Treatment of Infantile Hemangiomas.Clin Cosmet Investig Dermatol. 2021 Sep 3;14:1155-1163. doi: 10.2147/CCID.S332625. eCollection 2021. Clin Cosmet Investig Dermatol. 2021. PMID: 34511960 Free PMC article. Review.
-
Three-Dimensional Microtumor Formation of Infantile Hemangioma-Derived Endothelial Cells for Mechanistic Exploration and Drug Screening.Pharmaceuticals (Basel). 2022 Nov 12;15(11):1393. doi: 10.3390/ph15111393. Pharmaceuticals (Basel). 2022. PMID: 36422523 Free PMC article.
-
Comparison of efficacy and safety between oral propranolol combined with and without intralesional injection of lauromacrogol for infantile hemangioma.Front Pediatr. 2024 Jun 26;12:1361105. doi: 10.3389/fped.2024.1361105. eCollection 2024. Front Pediatr. 2024. PMID: 38989270 Free PMC article.
-
Expression of Cathepsins B, D, and G in Extracranial Arterio-Venous Malformation.Front Surg. 2021 Aug 2;8:676871. doi: 10.3389/fsurg.2021.676871. eCollection 2021. Front Surg. 2021. PMID: 34409065 Free PMC article.
-
Progress in the treatment of infantile hemangioma.Ann Transl Med. 2019 Nov;7(22):692. doi: 10.21037/atm.2019.10.47. Ann Transl Med. 2019. PMID: 31930093 Free PMC article. Review.
References
-
- Vishvanath A, Itinteang T, Tan ST, Day DJ. Infantile haemangioma expresses tumour necrosis factor-related apoptosis-inducing ligand (TRAIL), TRAIL receptors, osteoprotegerin and receptor activator for nuclear factor κB ligand (RANKL). Histopathology (2011) 59(3):397–406.10.1111/j.1365-2559.2011.03970.x - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources