

Impact of General Anesthesia on Safety and Outcomes in the Endovascular Arm of Interventional Management of Stroke (IMS) III Trial
- PMID: 26138125
- PMCID: PMC4519363
- DOI: 10.1161/STROKEAHA.115.008761
Impact of General Anesthesia on Safety and Outcomes in the Endovascular Arm of Interventional Management of Stroke (IMS) III Trial
Abstract
Background and purpose: General anesthesia (GA) for endovascular therapy (EVT) of acute ischemic stroke may be associated with worse outcomes.
Methods: The Interventional Management of Stroke III trial randomized patients within 3 hours of acute ischemic stroke onset to intravenous tissue-type plasminogen activator±EVT. GA use within 7 hours of stroke onset was recorded per protocol. Good outcome was defined as 90-day modified Rankin Scale ≤2. A multivariable analysis adjusting for dichotomized National Institutes of Health Stroke Scale (NIHSS; 8-19 versus ≥20), age, and time from onset to groin puncture was performed.
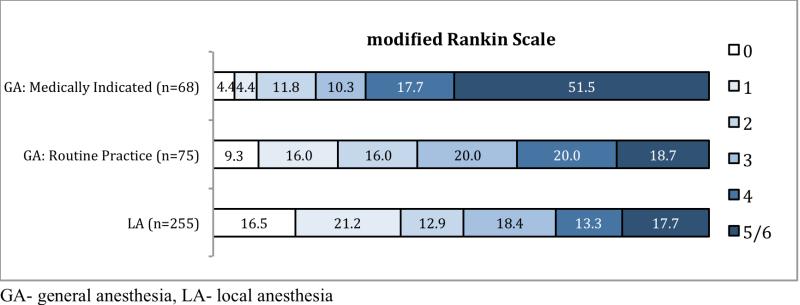
Results: Four hundred thirty-four patients were randomized to EVT, 269 (62%) were treated under local anesthesia and 147 (33.9%) under GA; 18 (4%) were undetermined. The 2 groups were comparable except for median baseline NIHSS (16 local anesthesia versus 18 GA; P<0.0001). The GA group was less likely to achieve a good outcome (adjusted relative risk, 0.68; confidence interval, 0.52-0.90; P=0.0056) and had increased in-hospital mortality (adjusted relative risk, 2.84; confidence interval, 1.65-4.91; P=0.0002). Those with medically indicated GA had worse outcomes (adjusted relative risk, 0.49; confidence interval, 0.30-0.81; P=0.005) and increased mortality (relative risk, 3.93; confidence interval, 2.18-7.10; P<0.0001) with a trend for higher mortality with routine GA. There was no significant difference in the adjusted risks of subarachnoid hemorrhage (P=0.32) or symptomatic intracerebral hemorrhage (P=0.37).
Conclusions: GA was associated with worse neurological outcomes and increased mortality in the EVT arm; this was primarily true among patients with medical indications for GA. Relative risk estimates, though not statistically significant, suggest reduced risk for subarachnoid hemorrhage and symptomatic intracerebral hemorrhage under local anesthesia. Although the reasons for these associations are not clear, these data support the use of local anesthesia when possible during EVT.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00359424.
Keywords: anesthesia; embolectomy; endovascular procedures; injections, intra-arterial; stroke; thrombolysis.
© 2015 American Heart Association, Inc.
Figures
Comment in
-
Use of General Anesthesia for Emergent Large Vessel Occlusion Patients.World Neurosurg. 2015 Dec;84(6):1498-500. doi: 10.1016/j.wneu.2015.10.028. Epub 2015 Oct 22. World Neurosurg. 2015. PMID: 26481338 No abstract available.
References
-
- Adams HP, Jr., del ZG, Alberts MJ, Bhatt DL, Brass L, Furlan A, et al. Guidelines for the early management of adults with ischemic stroke: A guideline from the american heart association/american stroke association stroke council, clinical cardiology council, cardiovascular radiology and intervention council, and the atherosclerotic peripheral vascular disease and quality of care outcomes in research interdisciplinary working groups: The american academy of neurology affirms the value of this guideline as an educational tool for neurologists. Stroke. 2007;38:1655–1711. - PubMed
-
- Abou-Chebl A, Lin R, Hussain MS, Jovin TG, Levy EI, Liebeskind DS, et al. Conscious sedation versus general anesthesia during endovascular therapy for acute anterior circulation stroke: Preliminary results from a retrospective, multicenter study. Stroke. 2010;41:1175–1179. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
