

Complications in Stent-Assisted Endovascular Therapy of Ruptured Intracranial Aneurysms and Relevance to Antiplatelet Administration: A Systematic Review
- PMID: 26138136
- PMCID: PMC7968784
- DOI: 10.3174/ajnr.A4365
Complications in Stent-Assisted Endovascular Therapy of Ruptured Intracranial Aneurysms and Relevance to Antiplatelet Administration: A Systematic Review
Abstract
Background and purpose: Despite the increasing use of stent-assisted coiling for ruptured intracranial aneurysms, there is little consensus regarding the appropriate antiplatelet administration for this. The objectives of this systematic review were to provide an overview of complications and their association with the method of antiplatelet administration in stent-assisted coiling for ruptured intracranial aneurysms.
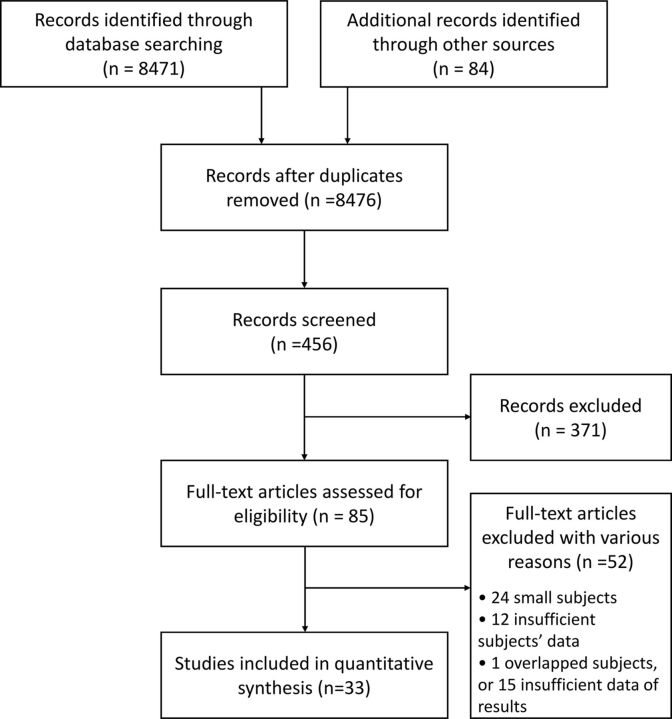
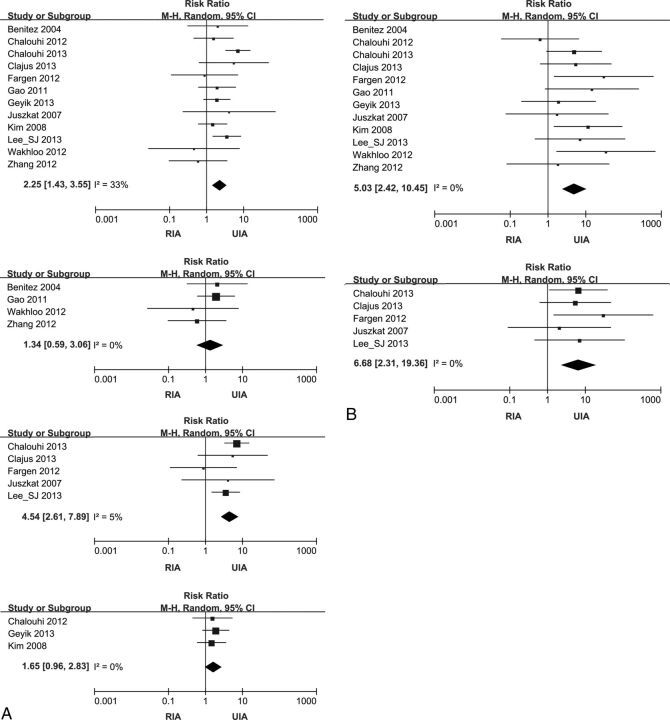
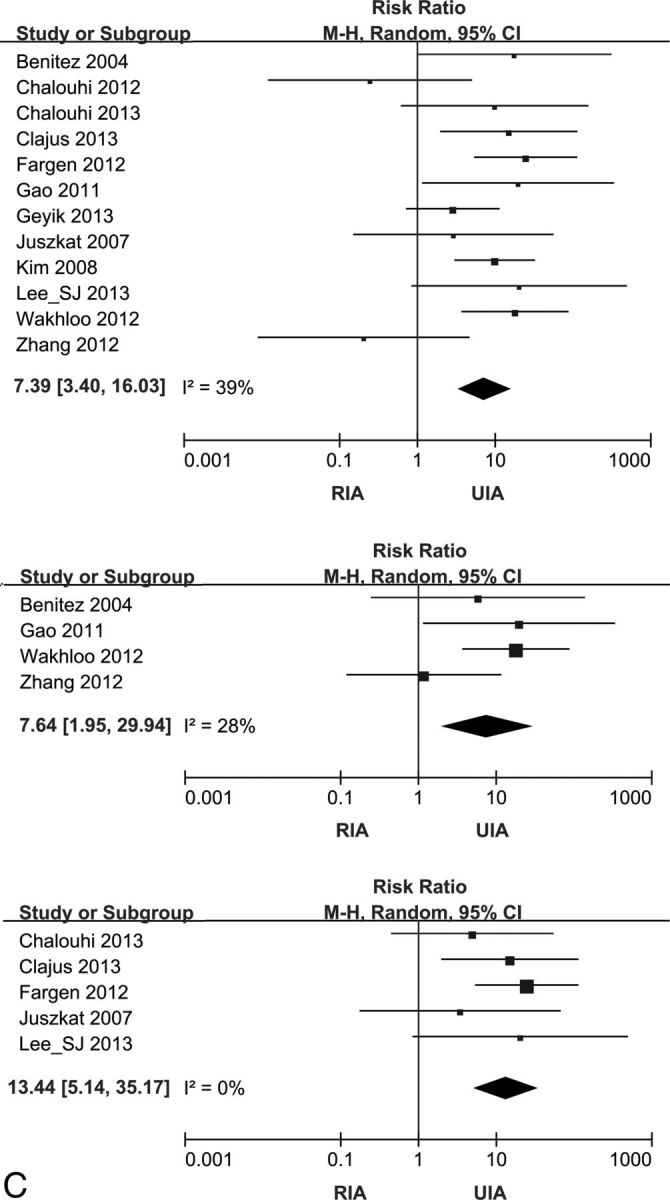
Materials and methods: A comprehensive search of the literature in the data bases was conducted to identify studies reporting complications of stent-assisted coiling for ruptured intracranial aneurysms. The pooled event rate of preprocedural thromboembolisms, hemorrhages, and mortality was estimated from the selected studies. Subgroup analyses were performed by the method of antiplatelet administration (pre-, postprocedural, and modified). Meta-analysis was conducted to compare periprocedural complications and mortality between ruptured intracranial aneurysms and unruptured intracranial aneurysms.
Results: Of the 8476 studies identified, 33 with 1090 patients were included. The event rates of thromboembolism and intra- and postprocedural hemorrhage were 11.2% (95% CI, 9.2%-13.6%), 5.4% (95% CI, 4.1%-7.2%), and 3.6% (95% CI, 2.6%-5.1%), respectively. Subgroup analyses of thromboembolism showed a statistically significant difference between groups (P < .05). In the preprocedural and modified antiplatelet groups, the risk for thromboembolism in stent-assisted coiling for ruptured intracranial aneurysm was not significantly different from that for unruptured intracranial aneurysm, though this risk of the postprocedural antiplatelet group was significantly higher in ruptured intracranial aneurysms than in unruptured intracranial aneurysms.
Conclusions: On the basis of current evidence, complications of stent-assisted coiling for ruptured intracranial aneurysm may be affected by the method of antiplatelet administration.
© 2015 by American Journal of Neuroradiology.
Figures
References
-
- Hwang G, Kim JG, Song KS, et al. . Delayed ischemic stroke after stent-assisted coil placement in cerebral aneurysm: characteristics and optimal duration of preventative dual antiplatelet therapy. Radiology 2014;273:194–201 - PubMed
-
- Zhang XD, Wu HT, Zhu J, et al. . Delayed intracranial hemorrhage associated with antiplatelet therapy in stent-assisted coil embolized cerebral aneurysms. Acta Neurochir Suppl 2011;110(pt 2):133–39 - PubMed
-
- Manabe H. Ruptured cerebral aneurysms treated by stent-assisted GDC embolization–two case reports with long-term follow-up. Acta Neurochir Suppl 2008;103:5–8 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical