

Sympathetic baroreflex gain in normotensive pregnant women
- PMID: 26139215
- PMCID: PMC4556837
- DOI: 10.1152/japplphysiol.00131.2015
Sympathetic baroreflex gain in normotensive pregnant women
Abstract
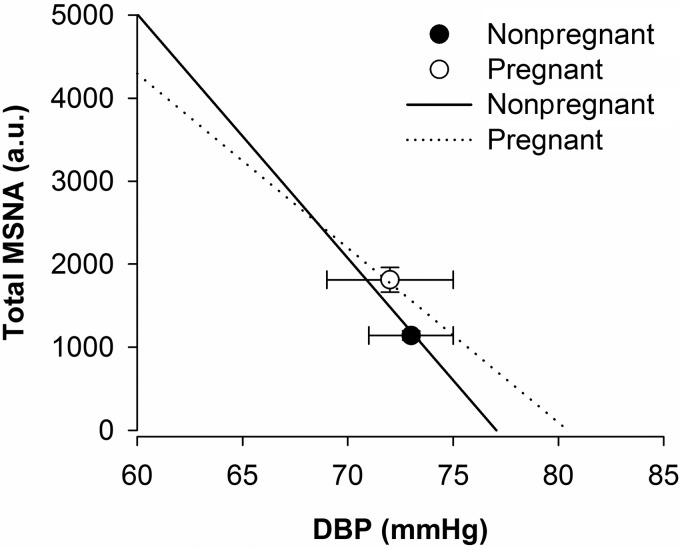
Muscle sympathetic nerve activity is increased during normotensive pregnancy while mean arterial pressure is maintained or reduced, suggesting baroreflex resetting. We hypothesized spontaneous sympathetic baroreflex gain would be reduced in normotensive pregnant women relative to nonpregnant matched controls. Integrated muscle sympathetic burst incidence and total sympathetic activity (microneurography), blood pressure (Finometer), and R-R interval (ECG) were assessed at rest in 11 pregnant women (33 ± 1 wk gestation, 31 ± 1 yr, prepregnancy BMI: 23.5 ± 0.9 kg/m(2)) and 11 nonpregnant controls (29 ± 1 yr; BMI: 25.2 ± 1.7 kg/m(2)). Pregnant women had elevated baseline sympathetic burst incidence (43 ± 2 vs. 33 ± 2 bursts/100 heart beats, P = 0.01) and total sympathetic activity (1,811 ± 148 vs. 1,140 ± 55 au, P < 0.01) relative to controls. Both mean (88 ± 3 vs. 91 ± 2 mmHg, P = 0.4) and diastolic (DBP) (72 ± 3 vs. 73 ± 2 mmHg, P = 0.7) pressures were similar between pregnant and nonpregnant women, respectively, indicating an upward resetting of the baroreflex set point with pregnancy. Baroreflex gain, calculated as the linear relationship between sympathetic burst incidence and DBP, was reduced in pregnant women relative to controls (-3.7 ± 0.5 vs. -5.4 ± 0.5 bursts·100 heart beats(-1)·mmHg(-1), P = 0.03), as was baroreflex gain calculated with total sympathetic activity (-294 ± 24 vs. -210 ± 24 au·100 heart beats(-1)·mmHg(-1); P = 0.03). Cardiovagal baroreflex gain (sequence method) was not different between nonpregnant controls and pregnant women (49 ± 8 vs. 36 ± 8 ms/mmHg; P = 0.2). However, sympathetic (burst incidence) and cardiovagal gains were negatively correlated in pregnant women (R = -0.7; P = 0.02). Together, these data indicate that the influence of the sympathetic nervous system over arterial blood pressure is reduced in normotensive pregnancy, in terms of both long-term and beat-to-beat regulation of arterial pressure, likely through a baroreceptor-dependent mechanism.
Keywords: baroreflex control; blood pressure; pregnancy; sympathetic nerve activity.
Copyright © 2015 the American Physiological Society.
Figures



References
-
- Barron WM, Mujais SK, Zinaman M, Bravo EL, Lindheimer MD. Plasma catecholamine responses to physiologic stimuli in normal human pregnancy. Am J Obstet Gynecol 154: 80–84, 1986. - PubMed
-
- Blaber AP, Yamamoto Y, Hughson RL. Methodology of spontaneous baroreflex relationship assessed by surrogate data analysis. Am J Physiol Heart Circ Physiol 268: H1682–H1687, 1995. - PubMed
-
- Blake MJ, Martin A, Manktelow BN, Armstrong C, Halligan AW, Panerai RB, Potter JF. Changes in baroreceptor sensitivity for heart rate during normotensive pregnancy and the puerperium. Clin Sci (Lond) 98: 259–268, 2000. - PubMed
-
- Brooks VL, Quesnell RR, Cumbee SR, Bishop VS. Pregnancy attenuates activity of the baroreceptor reflex. Clin Exp Pharmacol Physiol 22: 152–156, 1995. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources