

Cardiovascular magnetic resonance feature-tracking assessment of myocardial mechanics: Intervendor agreement and considerations regarding reproducibility
- PMID: 26139384
- PMCID: PMC4683162
- DOI: 10.1016/j.crad.2015.05.006
Cardiovascular magnetic resonance feature-tracking assessment of myocardial mechanics: Intervendor agreement and considerations regarding reproducibility
Abstract
Aim: To assess intervendor agreement of cardiovascular magnetic resonance feature tracking (CMR-FT) and to study the impact of repeated measures on reproducibility.
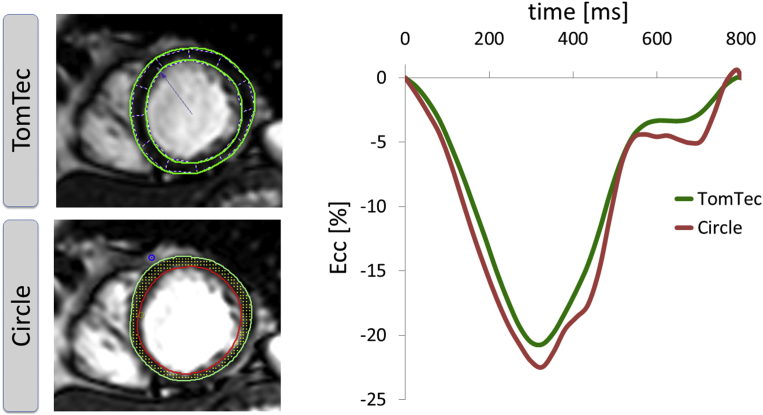
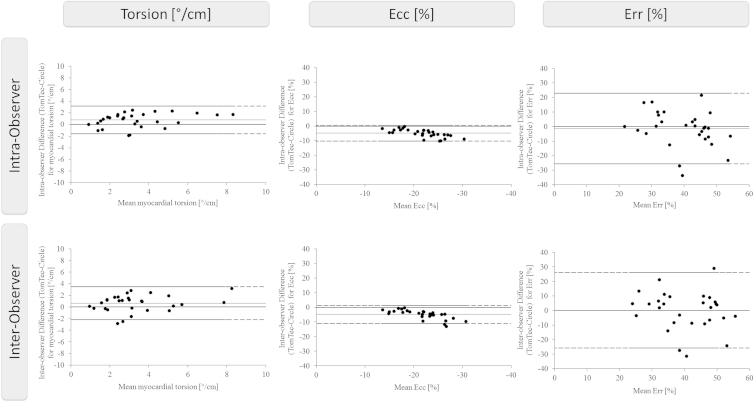
Materials and methods: Ten healthy volunteers underwent cine imaging in short-axis orientation at rest and with dobutamine stimulation (10 and 20 μg/kg/min). All images were analysed three times using two types of software (TomTec, Unterschleissheim, Germany and Circle, cvi(42), Calgary, Canada) to assess global left ventricular circumferential (Ecc) and radial (Err) strains and torsion. Differences in intra- and interobserver variability within and between software types were assessed based on single and averaged measurements (two and three repetitions with subsequent averaging of results, respectively) as determined by Bland-Altman analysis, intraclass correlation coefficients (ICC), and coefficient of variation (CoV).
Results: Myocardial strains and torsion significantly increased on dobutamine stimulation with both types of software (p<0.05). Resting Ecc and torsion as well as Ecc values during dobutamine stimulation were lower measured with Circle (p<0.05). Intra- and interobserver variability between software types was lowest for Ecc (ICC 0.81 [0.63-0.91], 0.87 [0.72-0.94] and CoV 12.47% and 14.3%, respectively) irrespective of the number of analysis repetitions. Err and torsion showed higher variability that markedly improved for torsion with repeated analyses and to a lesser extent for Err. On an intravendor level TomTec showed better reproducibility for Ecc and torsion and Circle for Err.
Conclusions: CMR-FT strain and torsion measurements are subject to considerable intervendor variability, which can be reduced using three analysis repetitions. For both vendors, Ecc qualifies as the most robust parameter with the best agreement, albeit lower Ecc values obtained using Circle, and warrants further investigation of incremental clinical merit.
Copyright © 2015 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved.
Figures


References
-
- Murray C.J., Lopez A.D. Alternative projections of mortality and disability by cause 1990-2020: Global Burden of Disease Study. Lancet. 1997;349:1498–1504. - PubMed
-
- Owan T.E., Hodge D.O., Herges R.M. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. - PubMed
-
- Karamitsos T.D., Francis J.M., Myerson S. The role of cardiovascular magnetic resonance imaging in heart failure. J Am Coll Cardiol. 2009;54:1407–1424. - PubMed
-
- Kowallick J.T., Edelmann F., Lotz J. Imaging diastolic dysfunction with cardiovascular magnetic resonance. J Cardiol Ther. 2014;1:58–64.
-
- Pennell D.J. Cardiovascular magnetic resonance. Circulation. 2010;121:692–705. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
