

Intrauterine administration of human chorionic gonadotropin does not improve pregnancy and life birth rates independently of blastocyst quality: a randomised prospective study
- PMID: 26141379
- PMCID: PMC4491277
- DOI: 10.1186/s12958-015-0069-1
Intrauterine administration of human chorionic gonadotropin does not improve pregnancy and life birth rates independently of blastocyst quality: a randomised prospective study
Abstract
Background: Successful embryo implantation depends on a well-timed maternal-embryonic crosstalk. Human chorionic gonadotropin (hCG) secreted by the embryo is known to play a key role in this process and to trigger a complex signal transduction cascade allowing the apposition, attachment, and invasion of the embryo into the decidualized uterus. Production of hCG was reported to be dependent on blastocyst quality and several articles suggested that intrauterine hCG injection increases pregnancy and implantation rates in IVF patients. However, no study has as yet analysed birth rates as final outcome. Our objective was to determine whether clinical outcome after blastocyst transfer can be improved by intrauterine injection of hCG and whether this is dependent on blastocyst quality.
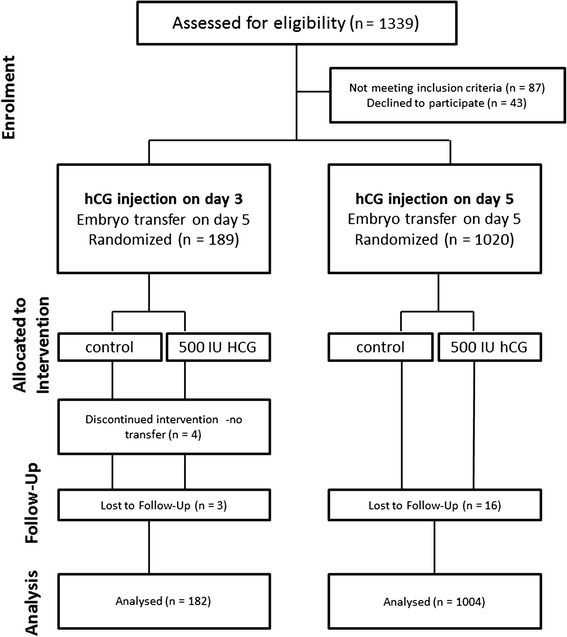
Methods: A prospective randomised study was conducted in two settings. In cohort A, hCG application was performed two days before blastocyst transfer. In cohort B, the administration of hCG occurred just prior to embryo transfer on day 5. For both cohorts, patients were randomised to either intrauterine hCG application or to the control group that received culture medium. Clinical outcome was analysed according to blastocyst quality of transferred embryos.
Results: The outcome of 182 IVF-cycles (cohort A) and 1004 IVF-cycles (cohort B) was analysed. All patients received a fresh autologous blastocyst transfer on day five. Primary outcomes were pregnancy rates (PR), clinical pregnancy rates (cPR), miscarriage rates (MR), and live birth rates (LBR). No improvement of clinical outcome after intrauterine hCG administration on day 3 (cohort A) or day 5 (cohort B) was found, independently of blastocyst quality transferred. The final outcome in cohort A: LBR after transfer of top blastocysts was 50.0 % with hCG and 53.3 % in the control group. With non-top blastocysts, LBR of 17.1 % (hCG) and 18.2 % (control) were observed (n.s.). In cohort B, LBR with top blastocysts was 53.3 % (hCG) and 48.4 % (control), with non-top blastocysts it came to 28.7 % (hCG) and 35.0 % (control). The differences between the groups were statistically not significant. Furthermore, we investigated a possible benefit of hCG administration in correlation with female age. In both age groups (<38 years and ≥ 38 years) we found similar LBR after treatment with hCG vs. medium. A LBR of 47.1 % vs. 48.7 % was obtained in the younger group and 26.6 % vs. 30.8 % in the older group.
Conclusions: In contrast to previous studies indicating a substantial benefit from intrauterine hCG application in cleavage stage embryo transfers, in our study we could not find any evidence for improvement of clinical outcome in blastocyst transfer cycles, neither with top nor with non-top quality morphology.
Figures
References
-
- Fluhr H, Bischof-Islami D, Krenzer S, Licht P, Bischof P, Zygmunt M. Human chorionic gonadotropin stimulates matrix metalloproteinases-2 and −9 in cytotrophoblastic cells and decreases tissue inhibitor of metalloproteinases-1, −2, and −3 in decidualized endometrial stromal cells. Fertil Steril. 2008;90:1390–5. doi: 10.1016/j.fertnstert.2007.08.023. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
