

What's new in melanoma? Combination!
- PMID: 26141621
- PMCID: PMC4491255
- DOI: 10.1186/s12967-015-0582-1
What's new in melanoma? Combination!
Abstract
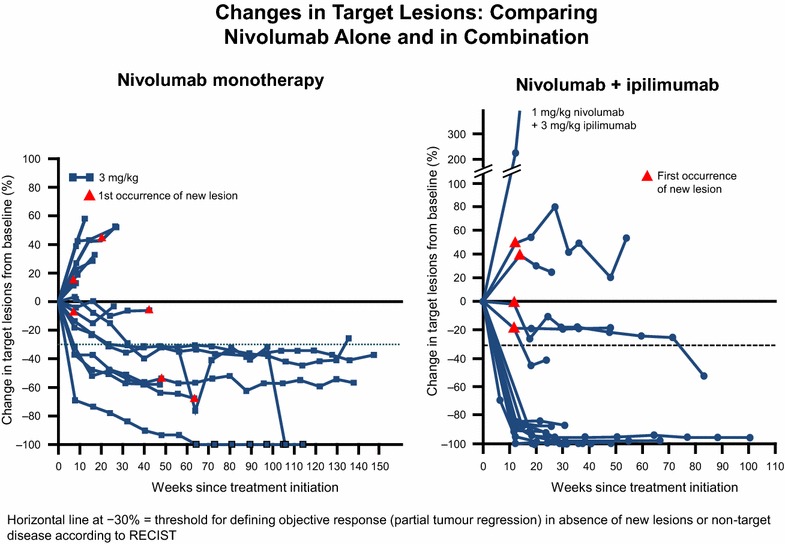
Melanoma was again a focus of attention at the 2015 American Society of Clinical Oncology (ASCO) Annual Meeting, in particular the use of combination treatment strategies involving immunotherapies and/or targeted agents. New data on targeted therapies confirmed previous findings, with combined BRAF inhibitor (vemurafenib) plus MEK inhibitor (cobimetinib) improving progression-free survival (PFS) compared to vemurafenib monotherapy in patients with BRAFV600 mutation-positive tumors (CoBRIM trial). Positive results were also seen with combined dabrafenib and trametinib in patients with BRAF V600E/K metastatic melanoma and encorafenib plus binimetinib in BRAFV600-mutant cutaneous melanoma. Even more interesting news centered on the use of combination immunotherapy, in particular the randomized, double-blind CheckMate 067 study in which median PFS with nivolumab plus ipilimumab was 11.5 months, compared to 2.9 months with ipilimumab alone (HR 0.42) and 6.9 months with nivolumab alone (HR 0.57). Of interest, in patients with ≥5% PD-L1 expression, median PFS was 14 months with the combination or with nivolumab alone compared with 3.9 months in the ipilimumab group, while in the PD-L1 negative cohort, the combination remained superior to both monotherapies. Given that combination therapy was accompanied by a high occurrence of side-effects, this raises the suggestion that combination therapy might be reserved for PD-L1 negative patients only, with PD-L1 positive patients achieving the same benefit from nivolumab monotherapy. However, overall survival data are awaited and the equivalence of single agent to the combination remains unconvincing. Interesting data were also reported on the combination of T-VEC (talimogene laherparepvec) with ipilimumab, and the anti-PD-1 agent MEDI4736 (durvolumab) combined with dabrafenib plus trametinib. Emerging data also suggested that predictive markers based on immunoprofiling and mismatch repair deficiency may be of clinical use. In conclusion, the use of combination approaches to treat patients with melanoma, as well as other cancers, is no longer a just a wish for the future but is today a clinical reality with a rapidly growing evidence-base. Moreover, the most exciting consideration is that this is far from the end of the story, but rather a fantastic introduction.
Figures
References
-
- Larkin JMG, Yan Y, McArthur GA, Ascierto PA, Liszkay G, Maio M et al (2015) Update of progression-free survival (PFS) and correlative biomarker analysis from coBRIM: phase III study of cobimetinib (cobi) plus vemurafenib (vem) in advanced BRAF-mutated melanoma. J Clin Oncol 33 (suppl; abstr 9006)
-
- Long GV, Stroyakovskiy D, Gogas H, Levchenko E, De Braud FG, Larkin JMG, et al (2015) Overall survival in COMBI-d, a randomized, double-blinded, phase III study comparing the combination of dabrafenib and trametinib with dabrafenib and placebo as first-line therapy in patients (pts) with unresectable or metastatic BRAF V600E/K mutation-positive cutaneous melanoma. J Clin Oncol 33 (suppl; abstr 102)
-
- Flaherty K, Daud A, Weber JS, Sosman JA, Kim K, Gonzalez R et al (2014) Updated overall survival (OS) for BRF113220, a phase 1–2 study of dabrafenib (D) alone versus combined dabrafenib and trametinib (D + T) in pts with BRAF V600 mutation-positive (+) metastatic melanoma (MM). J Clin Oncol 32:5s (suppl; abstr 9010^)
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
