

Patient-specific dose calculations for pediatric CT of the chest, abdomen and pelvis
- PMID: 26142256
- PMCID: PMC4623993
- DOI: 10.1007/s00247-015-3400-2
Patient-specific dose calculations for pediatric CT of the chest, abdomen and pelvis
Abstract
Background: Organ dose is essential for accurate estimates of patient dose from CT.
Objective: To determine organ doses from a broad range of pediatric patients undergoing diagnostic chest-abdomen-pelvis CT and investigate how these relate to patient size.
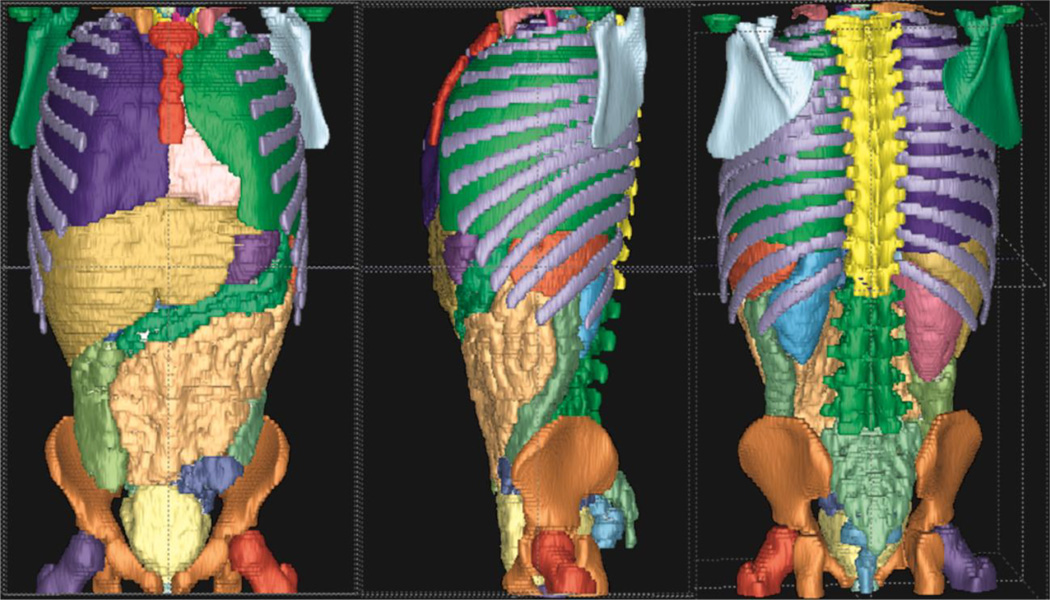
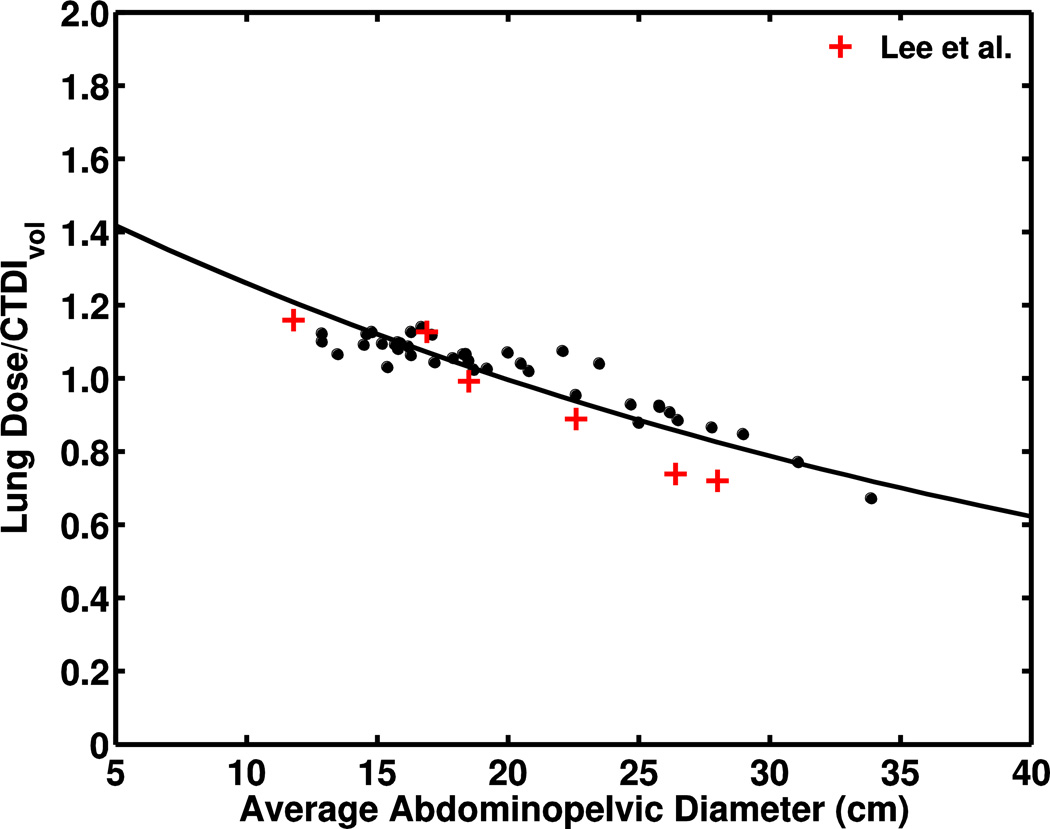
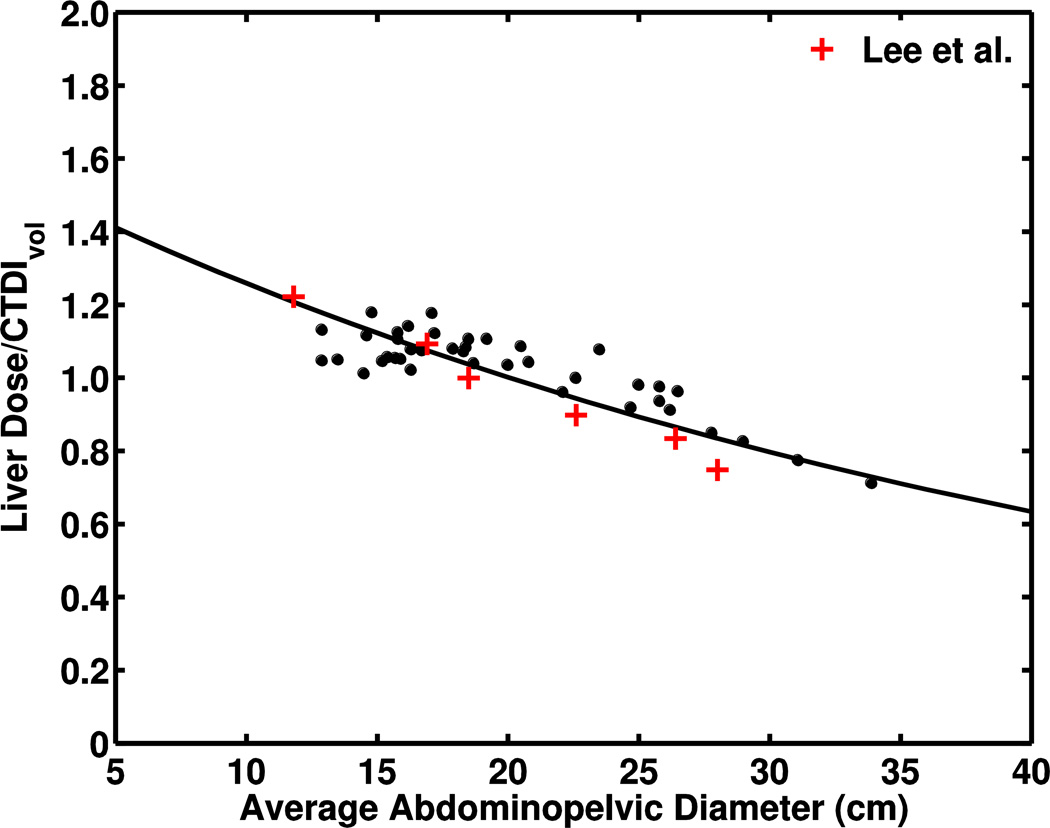
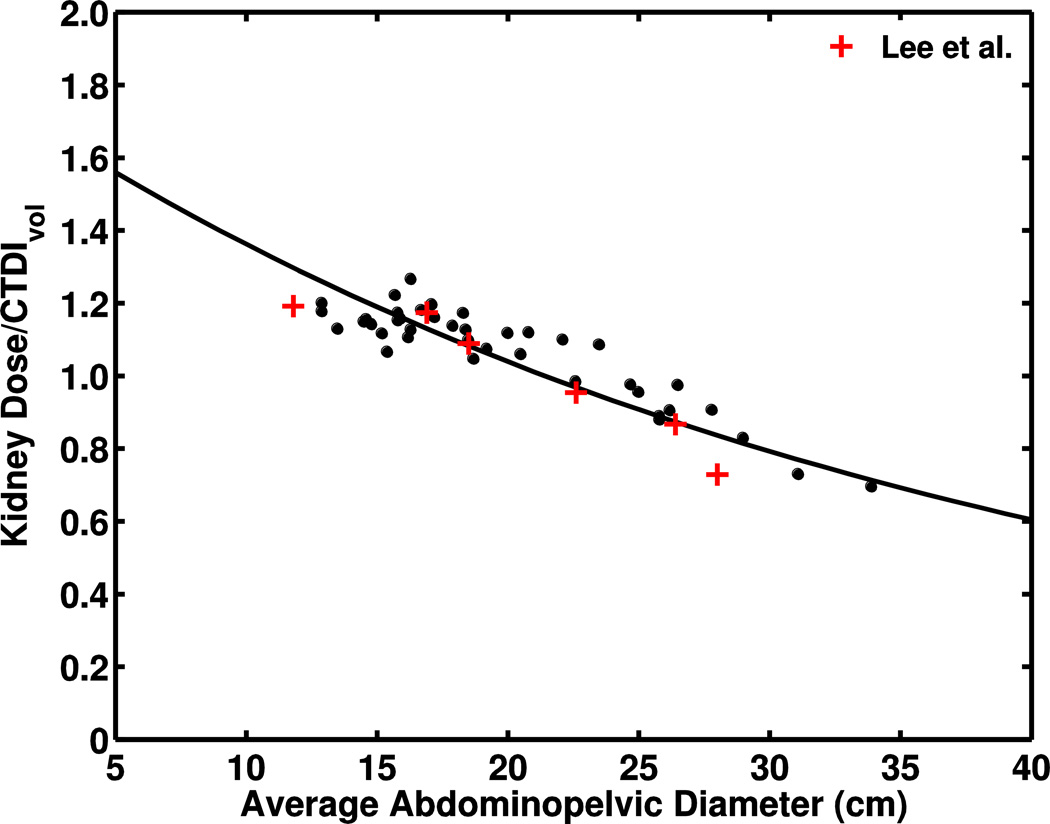
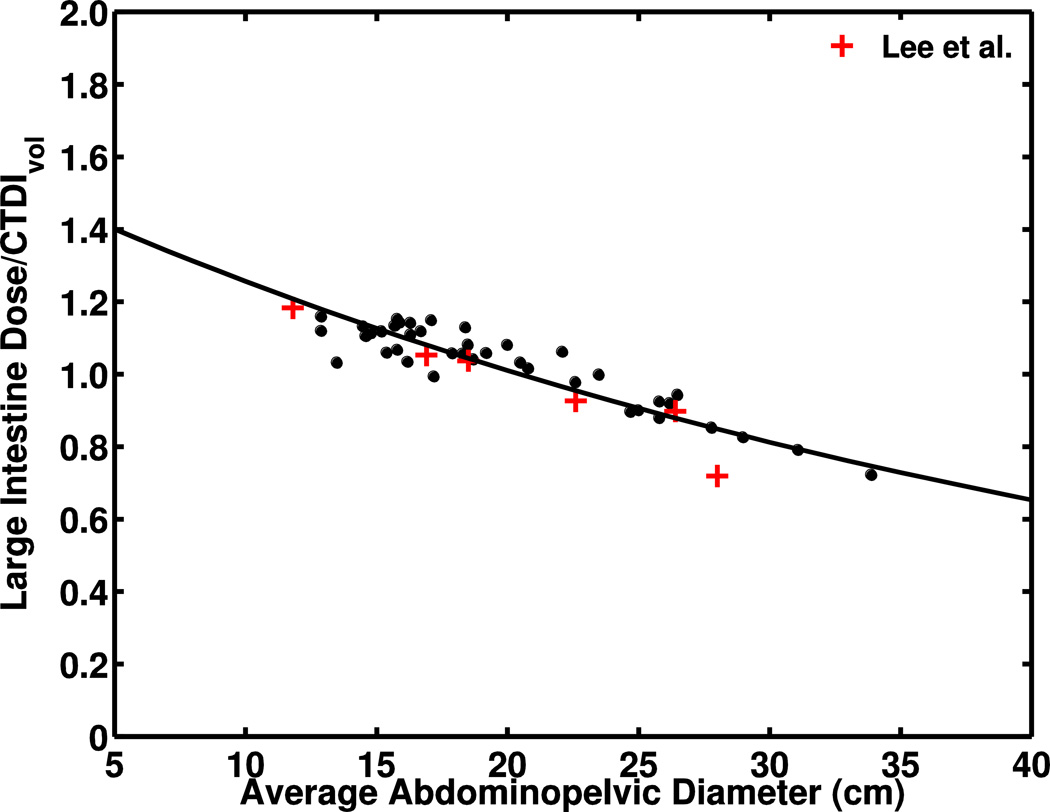
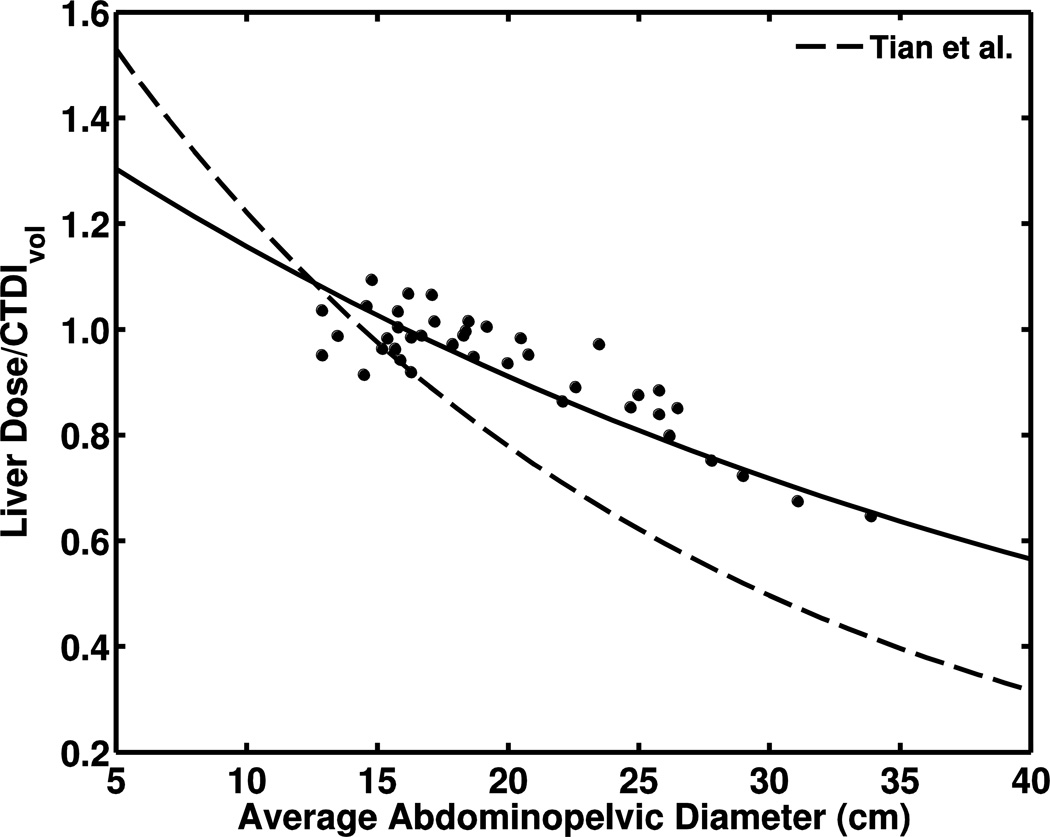
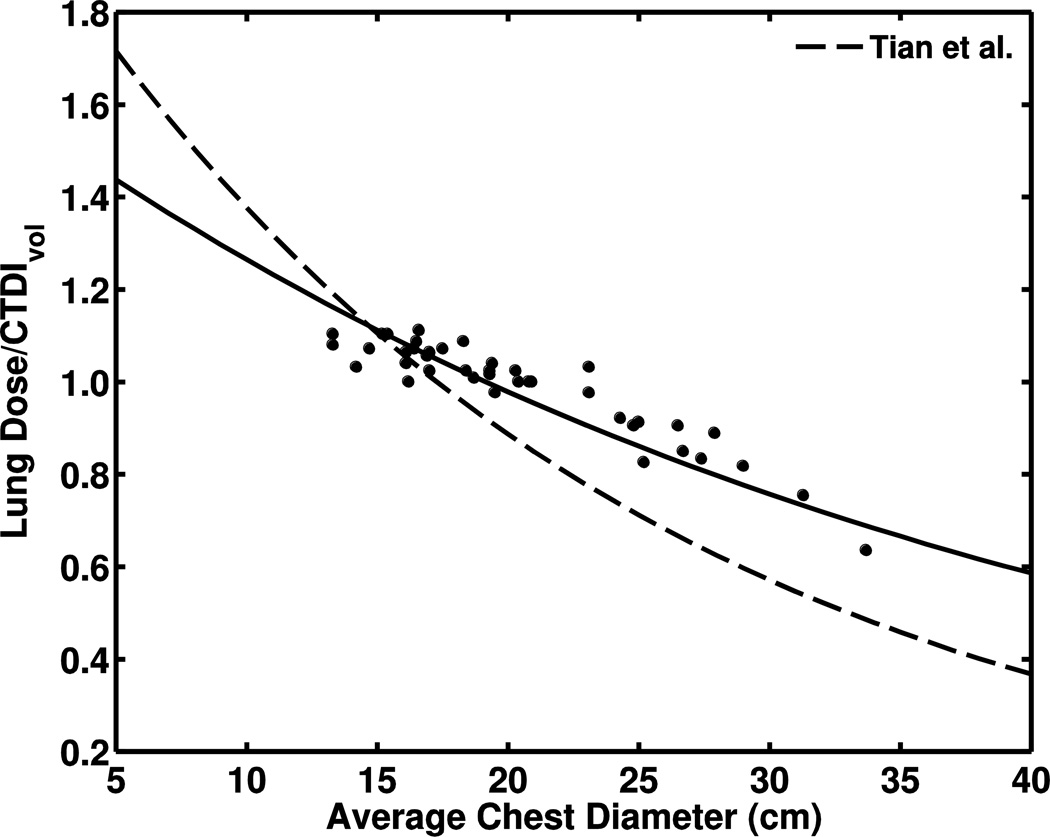
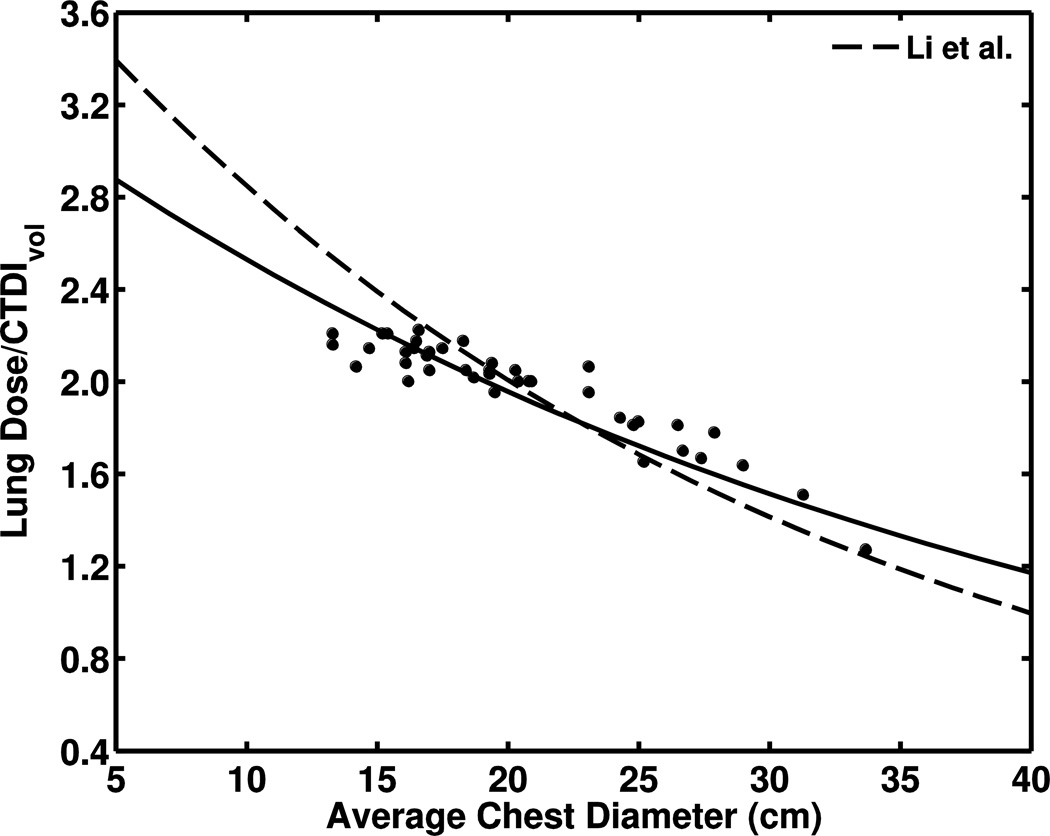
Materials and methods: We used a previously validated Monte Carlo simulation model of a Philips Brilliance 64 multi-detector CT scanner (Philips Healthcare, Best, The Netherlands) to calculate organ doses for 40 pediatric patients (M:F = 21:19; range 0.6-17 years). Organ volumes and positions were determined from the images using standard segmentation techniques. Non-linear regression was performed to determine the relationship between volume CT dose index (CTDIvol)-normalized organ doses and abdominopelvic diameter. We then compared results with values obtained from independent studies.
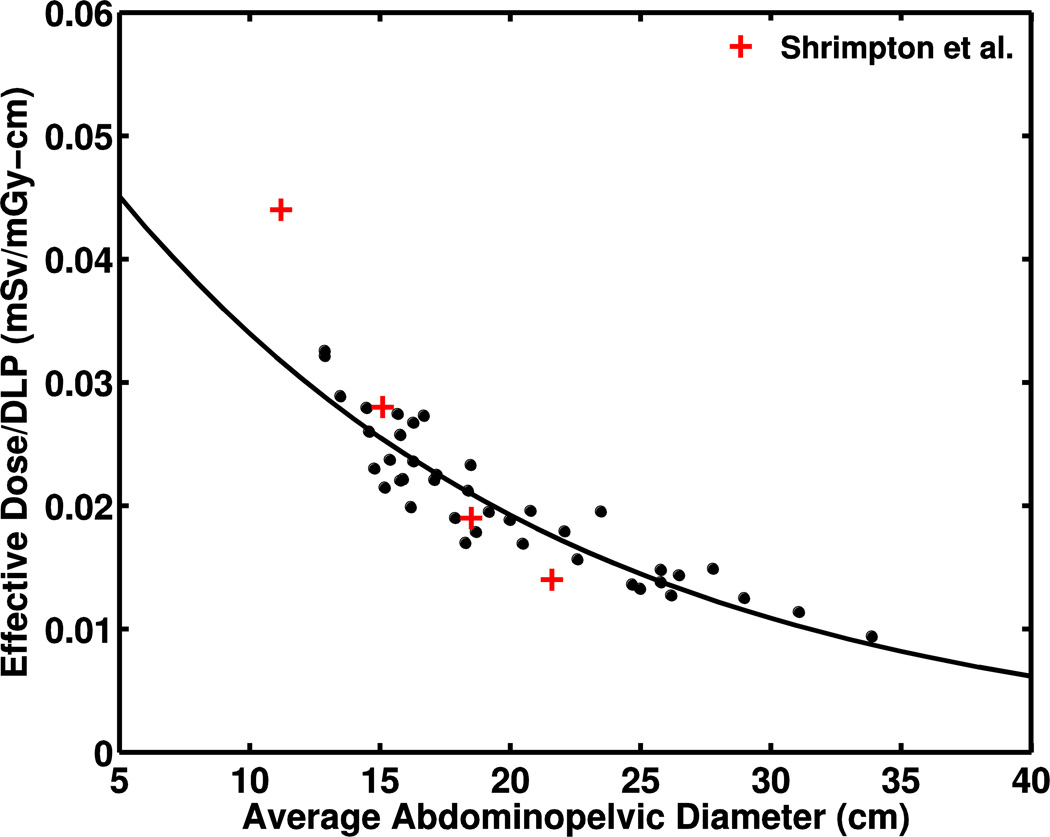
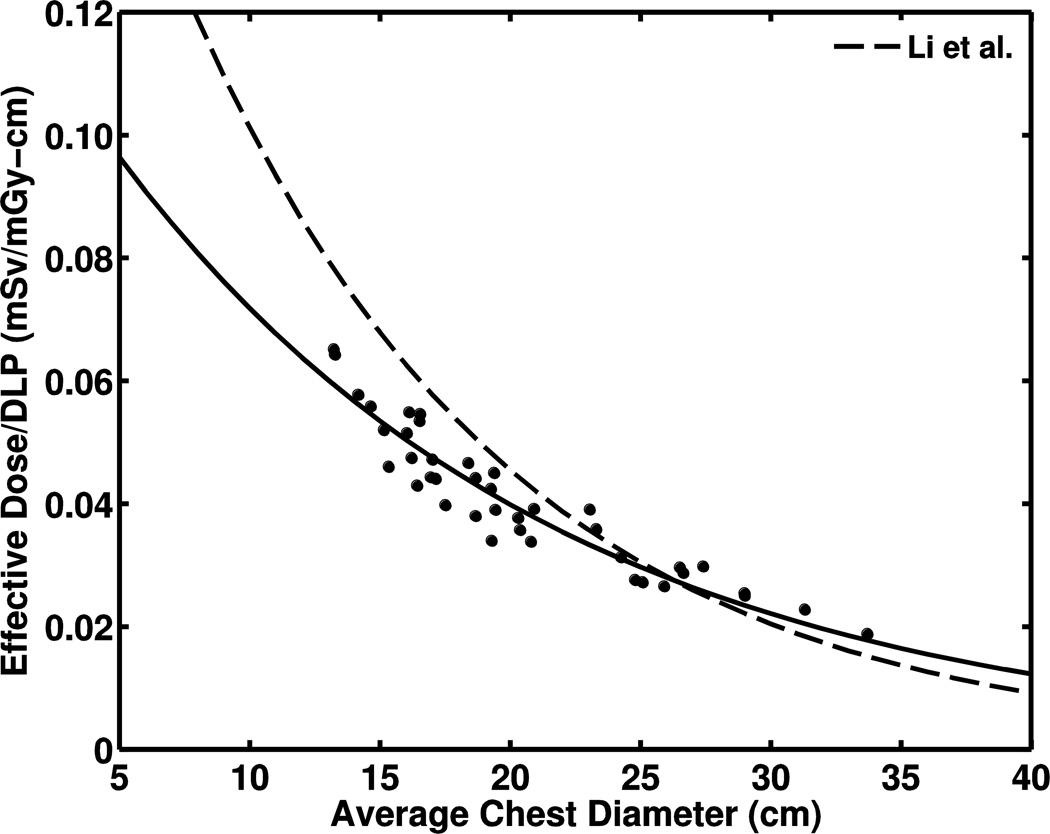
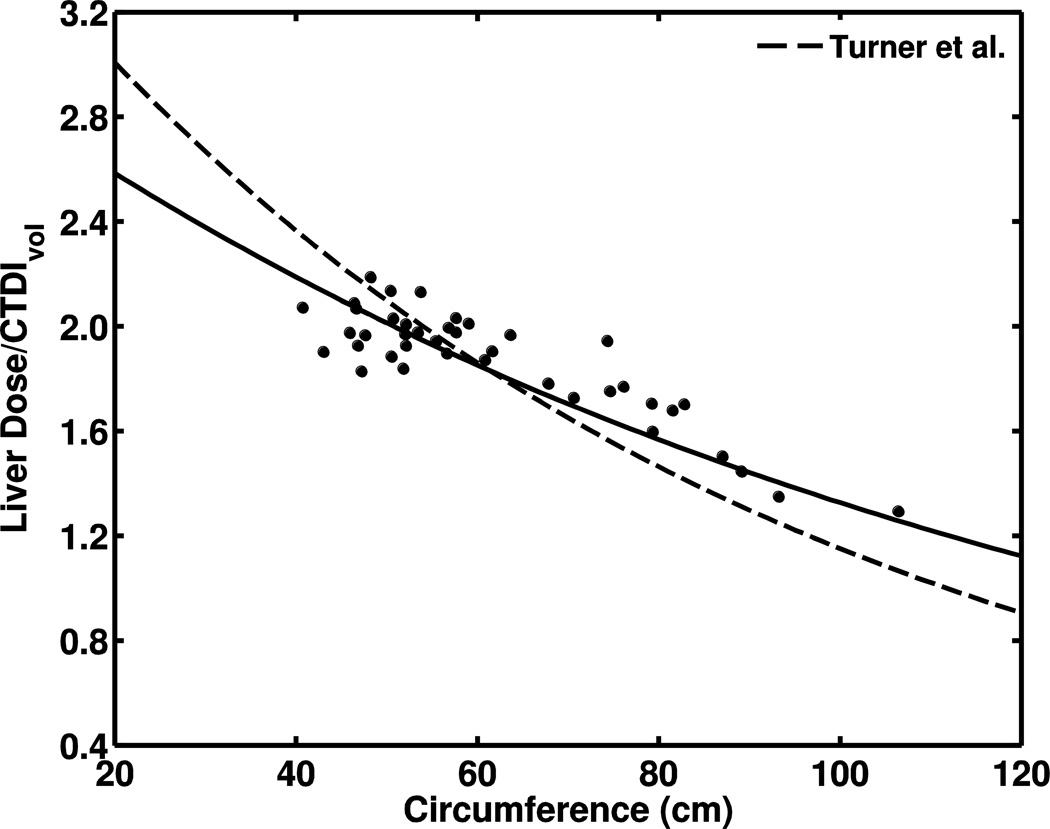
Results: We found that CTDIvol-normalized organ dose correlated strongly with exponentially decreasing abdominopelvic diameter (R(2) > 0.8 for most organs). A similar relationship was determined for effective dose when normalized by dose-length product (R(2) = 0.95). Our results agreed with previous studies within 12% using similar scan parameters (e.g., bowtie filter size, beam collimation); however results varied up to 25% when compared to studies using different bowtie filters.
Conclusion: Our study determined that organ doses can be estimated from measurements of patient size, namely body diameter, and CTDIvol prior to CT examination. This information provides an improved method for patient dose estimation.
Keywords: Children; Computed tomography; Effective dose; Monte Carlo; Organ dose; Patient size.
Conflict of interest statement
Figures
References
-
- National Council on Radiation Protection and Measurements. Ionizing radiation exposure of the population of the United States. NCRP Report No. 160. Bethesda, MD: National Council on Radiation Protection and Measurements; 2009.
-
- Paterson A, Frush D. Dose reduction in paediatric MDCT: general principles. Clin Radiol. 2007;62:507–517. - PubMed
-
- National Research Council. Health risks from exposure to low levels of ionising radiation: BEIR VII report. Washington, DC: 2006.
-
- Brenner DJ. Estimating cancer risks from pediatric CT: going from the qualitative to the quantitative. Pediatr Radiol. 2002;32:228–231. - PubMed
-
- Brenner DJ, Elliston CD, Hall EJ, Berdon WE. Estimated risks of radiation-induced fatal cancer from pediatric CT. AJR Am J Roentgenol. 2001;176:289–296. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
