

Pathophysiology and risk factors for osteonecrosis
- PMID: 26142896
- PMCID: PMC4596210
- DOI: 10.1007/s12178-015-9277-8
Pathophysiology and risk factors for osteonecrosis
Abstract
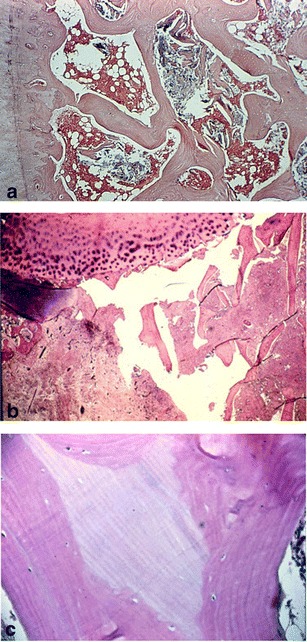
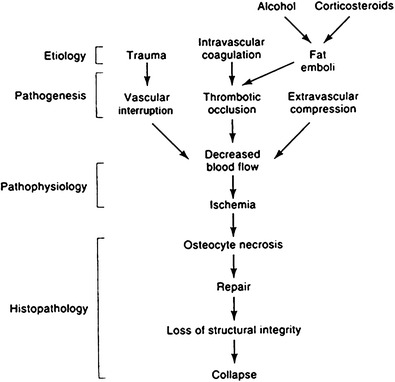
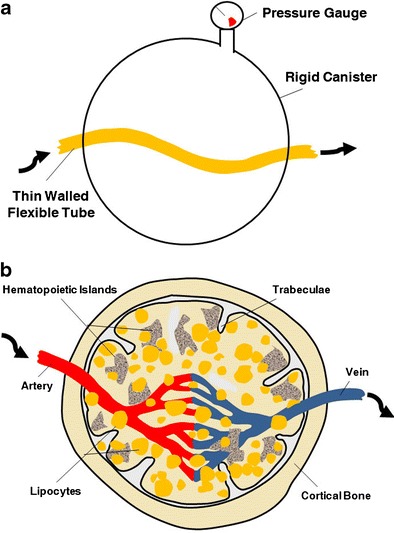
Osteonecrosis, also known as avascular necrosis or AVN, is characterized by a stereotypical pattern of cell death and a complex repair process of bone resorption and formation. It is not the necrosis itself but rather the resorptive component of the repair process that results in loss of structural integrity and subchondral fracture. Most likely, a common pathophysiological pathway exists involving compromised subchondral microcirculation. Decreased femoral head blood flow can occur through three mechanisms: vascular interruption by fractures or dislocation, intravascular occlusion from thrombi or embolic fat, or intraosseous extravascular compression from lipocyte hypertrophy or Gaucher cells. In this review, we emphasize etiologic relationships derived mostly from longitudinal cohort studies or meta-analyses whose causal relationships to osteonecrosis can be estimated with confidence. Understanding risk factors and pathophysiology has therapeutic implications since several treatment regimens are available to optimize femoral head circulation, interrupt bone resorption, and preserve the subchondral bone.
Figures
References
-
- Aaron RK, Gray R. Osteonecrosis: etiology, natural history, pathophysiology, and diagnosis. In: Callaghan JJ, Rosenberg AG, Rubash HE, editors. The adult hip. Philadelphia: Lippincott Williams & Wilkins; 2007. pp. 465–76.
-
- James J, Steijn-Myagkaya GL. Death of osteocytes. Electron microscopy after in vitro ischaemia. J Bone Joint Surg (Br) 1986;68(4):620–4. - PubMed
-
- Bauer TW, Stulberg BN, et al. The histology of osteonecrosis and its distinction from histologic artifacts. In: Schoutens A, et al., editors. Bone circulation and vascularization in normal and pathological conditions. New York: Plenum Press; 1993. pp. 283–92.
-
- Kenzora JE GM, et al. Osteonecrosis. In: Kelly WN HE, Ruddy S, et al., editors. Textbook of rheumatology. Philadelphia: WB Saunders; 1981. pp. 1755–82.
-
- Glimcher MJ, Kenzora JE. The biology of osteonecrosis of the human femoral head and its clinical implications: I. Tissue biology. Clin Orthop Relat Res. 1979;138:284–309. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
