

The Etiology and Pathogenesis of Chronic Rhinosinusitis: a Review of Current Hypotheses
- PMID: 26143392
- PMCID: PMC4874491
- DOI: 10.1007/s11882-015-0540-2
The Etiology and Pathogenesis of Chronic Rhinosinusitis: a Review of Current Hypotheses
Abstract
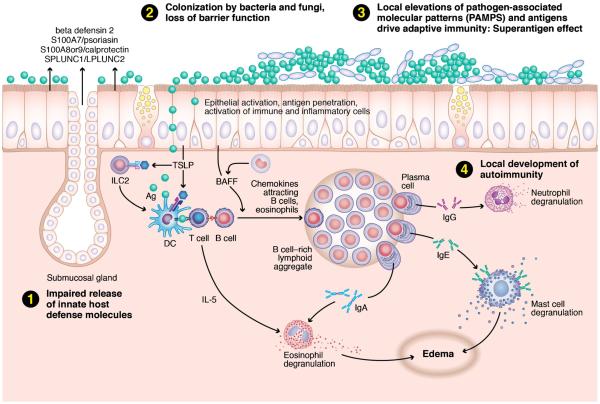
Chronic rhinosinusitis (CRS) is a broad clinical syndrome that is characterized by prolonged mucosal inflammation of the nose and paranasal sinuses, and is typically divided into two subtypes based on the presence or absence of nasal polyps. The etiology and pathogenesis of both forms remain areas of active research. Over the last 15 years, a number of hypotheses have been proposed to explain all or part of the clinical CRS spectrum. These hypotheses reflect the concept that CRS results from a dysfunctional interplay between individual host characteristics and factors exogenous to the host. Six broad theories on CRS etiology and pathogenesis are discussed as follows: (1) the "fungal hypothesis," (2) the "superantigen hypothesis," (3) the "biofilm hypothesis," and (4) the "microbiome hypothesis," all of which emphasize key environmental factors, and (5) the "eicosanoid hypothesis" and (6) the "immune barrier hypothesis," which describe specific host factors. These theories are reviewed, and the evidence supporting them is critically appraised.
Figures
References
-
- Fokkens WJ, Lund VJ, Mullol J, et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2012. Rhinol Suppl. 2012;3:1–298. p preceding table of contents. - PubMed
-
This is an updated and comprehensive reference document created by international collaboration that serves as the standard guideline for definitions, classifications, and diagnostic criteria for acute and chronic rhinosinusitis.
-
- Pleis JR, Lucas JW, Ward BW. Summary health statistics for U.S. adults: National Health Interview Survey, 2008. Vital Health Stat. 2009;10:1–157. - PubMed
-
- Jarvis D, Newson R, Lotvall J, et al. Asthma in adults and its association with chronic rhinosinusitis: the GA2LEN survey in Europe. Allergy. 2012;67:91–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
