

Is a threshold-based model a superior method to the relative percent concept for establishing individual exercise intensity? a randomized controlled trial
- PMID: 26146564
- PMCID: PMC4491229
- DOI: 10.1186/s13102-015-0011-z
Is a threshold-based model a superior method to the relative percent concept for establishing individual exercise intensity? a randomized controlled trial
Abstract
Background: Exercise intensity is arguably the most critical component of the exercise prescription model. It has been suggested that a threshold based model for establishing exercise intensity might better identify the lowest effective training stimulus for all individuals with varying fitness levels; however, experimental evidence is lacking. The purpose of this study was to compare the effectiveness of two exercise training programs for improving cardiorespiratory fitness: threshold based model vs. relative percent concept (i.e., % heart rate reserve - HRR).
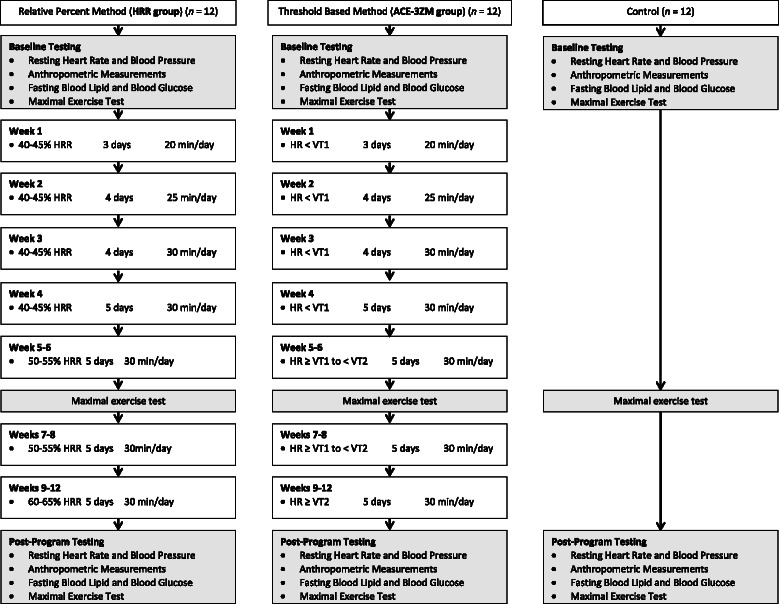
Methods: Apparently healthy, but sedentary men and women (n = 42) were randomized to a non-exercise control group or one of two exercise training groups. Exercise training was performed 30 min/day on 5 days/week for 12weeks according to one of two exercise intensity regimens: 1) a relative percent method was used in which intensity was prescribed according to percentages of heart rate reserve (HRR group), or 2) a threshold based method (ACE-3ZM) was used in which intensity was prescribed according to the first ventilatory threshold (VT1) and second ventilatory threshold (VT2).
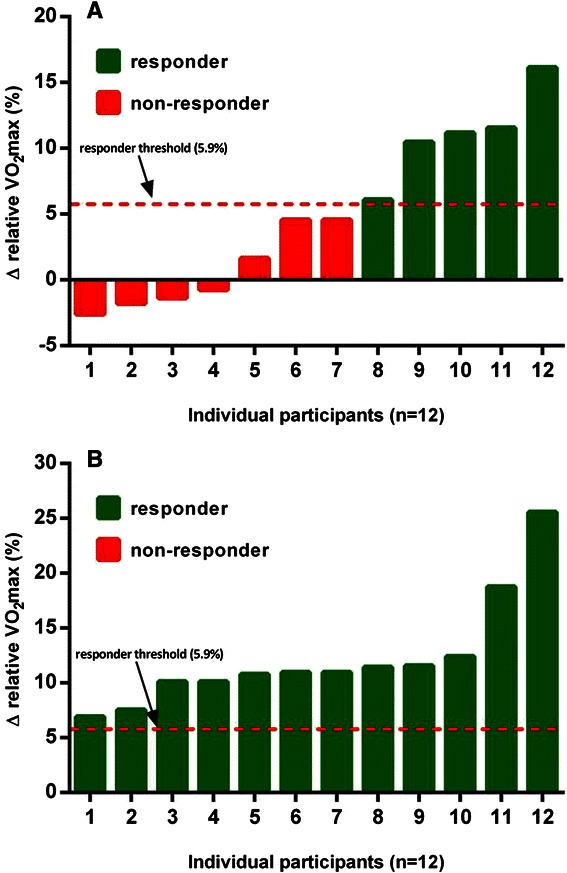
Results: Thirty-six men and women completed the study. After 12weeks, VO2max increased significantly (p < 0.05 vs. controls) in both HRR (1.76 ± 1.93 mL/kg/min) and ACE-3ZM (3.93 ± 0.96 mL/kg/min) groups. Repeated measures ANOVA identified a significant interaction between exercise intensity method and change in VO2max values (F = 9.06, p < 0.05) indicating that VO2max responded differently to the method of exercise intensity prescription. In the HRR group 41.7 % (5/12) of individuals experienced a favorable change in relative VO2max (Δ > 5.9 %) and were categorized as responders. Alternatively, exercise training in the ACE-3ZM group elicited a positive improvement in relative VO2max (Δ > 5.9 %) in 100 % (12/12) of the individuals.
Conclusions: A threshold based exercise intensity prescription: 1). elicited significantly (p < 0.05) greater improvements in VO2max, and 2). attenuated the individual variation in VO2max training responses when compared to relative percent exercise training. These novel findings are encouraging and provide important preliminary data for the design of individualized exercise prescriptions that will enhance training efficacy and limit training unresponsiveness.
Trial registration: ClinicalTrials.gov Identifier: ID NCT02351713 Registered 30 January 2015.
Keywords: Cardiorespiratory fitness; Cardiovascular Disease; Exercise prescription; Primary prevention; VO2max.
Figures
Similar articles
-
The incidence of training responsiveness to cardiorespiratory fitness and cardiometabolic measurements following individualized and standardized exercise prescription: study protocol for a randomized controlled trial.Trials. 2016 Dec 19;17(1):601. doi: 10.1186/s13063-016-1735-0. Trials. 2016. PMID: 27993169 Free PMC article. Clinical Trial.
-
Methods of prescribing relative exercise intensity: physiological and practical considerations.Sports Med. 2013 Jul;43(7):613-25. doi: 10.1007/s40279-013-0045-x. Sports Med. 2013. PMID: 23620244 Review.
-
Dose-response relationship of cardiorespiratory fitness adaptation to controlled endurance training in sedentary older adults.Eur J Prev Cardiol. 2016 Mar;23(5):518-29. doi: 10.1177/2047487315582322. Epub 2015 Apr 21. Eur J Prev Cardiol. 2016. PMID: 25901000
-
Changes in the Second Ventilatory Threshold Following Individualised versus Standardised Exercise Prescription among Physically Inactive Adults: A Randomised Trial.Int J Environ Res Public Health. 2022 Mar 26;19(7):3962. doi: 10.3390/ijerph19073962. Int J Environ Res Public Health. 2022. PMID: 35409646 Free PMC article. Clinical Trial.
-
Biological and methodological factors affecting response variability to endurance training and the influence of exercise intensity prescription.Exp Physiol. 2021 Jul;106(7):1410-1424. doi: 10.1113/EP089565. Epub 2021 Jun 8. Exp Physiol. 2021. PMID: 34036650 Review.
Cited by
-
Glycemic Threshold as an Alternative Method to Identify the Anaerobic Threshold in Patients With Type 2 Diabetes.Front Physiol. 2018 Nov 13;9:1609. doi: 10.3389/fphys.2018.01609. eCollection 2018. Front Physiol. 2018. PMID: 30483156 Free PMC article.
-
Insufficient exercise intensity for clinical benefit? Monitoring and quantification of a community-based Phase III cardiac rehabilitation programme: A United Kingdom perspective.PLoS One. 2019 Jun 13;14(6):e0217654. doi: 10.1371/journal.pone.0217654. eCollection 2019. PLoS One. 2019. PMID: 31194759 Free PMC article. Clinical Trial.
-
Acute effects of high-intensity interval training and moderate-intensity continuous training sessions on cardiorespiratory parameters in healthy young men.Eur J Appl Physiol. 2017 Jul;117(7):1437-1444. doi: 10.1007/s00421-017-3636-7. Epub 2017 May 9. Eur J Appl Physiol. 2017. PMID: 28488137 Clinical Trial.
-
The Effect of Detraining after a Period of Training on Cardiometabolic Health in Previously Sedentary Individuals.Int J Environ Res Public Health. 2018 Oct 19;15(10):2303. doi: 10.3390/ijerph15102303. Int J Environ Res Public Health. 2018. PMID: 30347735 Free PMC article.
-
The influence of protocol design on the identification of ventilatory thresholds and the attainment of peak physiological responses during synchronous arm crank ergometry in able-bodied participants.Eur J Appl Physiol. 2019 Oct;119(10):2275-2286. doi: 10.1007/s00421-019-04211-9. Epub 2019 Aug 21. Eur J Appl Physiol. 2019. PMID: 31435767 Free PMC article.
References
-
- Pescatello LS, editor. ACSM’s Guidelines for Exercise Testing and Prescription. 9. Baltimore, MD: Lippincott Williams & Wilkins; 2014.
-
- Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee I, Nieman DC. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43:1334–1359. doi: 10.1249/MSS.0b013e318213fefb. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
