

Laparoscopic colonic resection for splenic flexure cancer: our experience
- PMID: 26148781
- PMCID: PMC4494171
- DOI: 10.1186/s12876-015-0301-7
Laparoscopic colonic resection for splenic flexure cancer: our experience
Abstract
Background: The treatment of colon cancer located in splenic flexure is not standardized. Laparoscopic approach is still considered a challenging procedure. This study reviews two Institutions experience in laparoscopic treatment of left colonic flexure cancer. Intraoperative, pathologic and postoperative data from patients undergoing laparoscopic splenic flexure resection were analyzed to assess oncological safety as well as early and medium-term outcomes.
Methods: From October 2005 to May 2014 laparoscopic splenic flexure resection was performed in 23 patients.
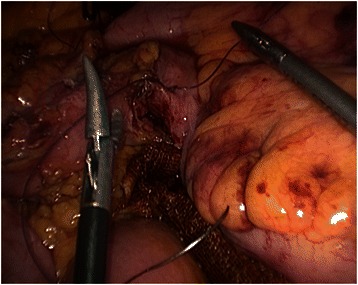
Results: Conversion rate was nihil. In 7 cases the anastomosis was performed intracorporeally. Specimen mean length was 21.2 cm, while the distance of distal and proximal resection margin from tumor site was 6.5 and 11.5 respectively. The mean number of harvested lymph nodes was 20.8. Mean operative time was 190 min and mean estimated blood loss was equal to 55 ml. As regard major postoperative complications, one case of postoperative acute pancreatitis and one case of postoperative bleeding from the anastomotic suture line were reported.
Conclusions: Although our experience is limited and appropriate indications must be set by future randomized studies, we believe that laparoscopic resection with intracorporeal anastomosis appears feasible and safe for patients affected by splenic flexure cancer.
Figures



References
-
- Jacobs M, Verdeja JC, Goldstein HS. Minimally invasive colon resection (laparoscopic colectomy) Surg Laparosc Endosc. 1991;1:144–50. - PubMed
-
- Guillou PJ, Quirke P, Thorpe H, Walker J, Jayne DG, Smith AM, Heath RM, Brown JM, MRC CLASICC trial group Short-term endpoint of conventional versus laparoscopic assisted surgery in patients with colorectal cancer: multicentre, randomised controlled trial. Lancet. 2005;365(9472):1718–26. doi: 10.1016/S0140-6736(05)66545-2. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
