

In situ vaccination by radiotherapy to improve responses to anti-CTLA-4 treatment
- PMID: 26148880
- PMCID: PMC4684480
- DOI: 10.1016/j.vaccine.2015.05.105
In situ vaccination by radiotherapy to improve responses to anti-CTLA-4 treatment
Abstract
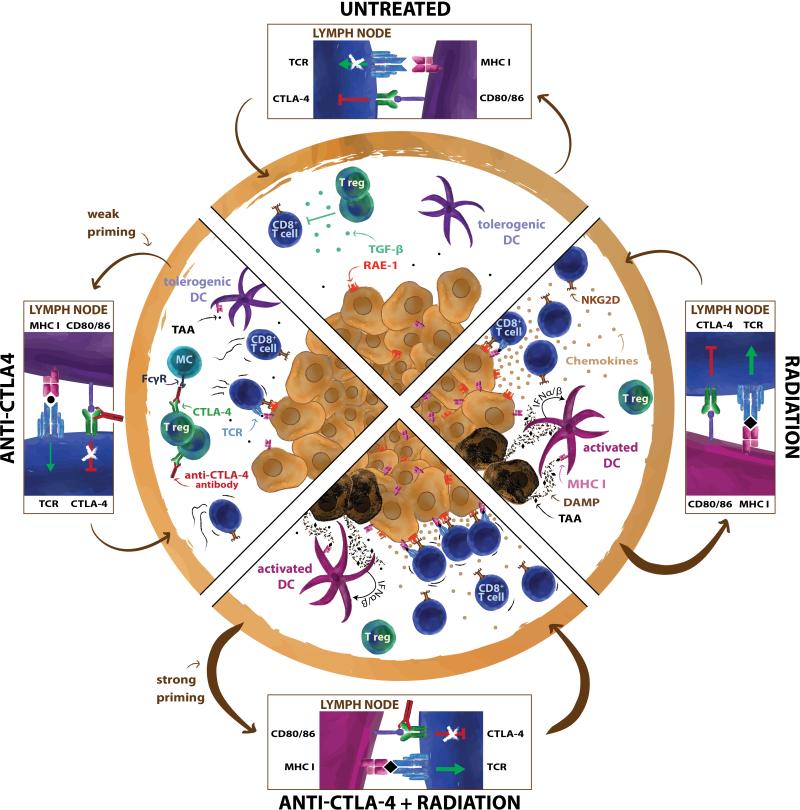
Targeting immune checkpoint receptors has emerged as an effective strategy to induce immune-mediated cancer regression in the subset of patients who have significant pre-existing anti-tumor immunity. For the remainder, effective anti tumor responses may require vaccination. Radiotherapy, traditionally used to achieve local tumor control, has acquired a new role, that of a partner for immunotherapy. Ionizing radiation has pro-inflammatory effects that facilitate tumor rejection. Radiation alters the tumor to enhance the concentration of effector T cells via induction of chemokines, cytokines and adhesion molecules. In parallel, radiation can induce an immunogenic death of cancer cells, promoting cross-presentation of tumor-derived antigens by dendritic cells to T cells. Newly generated anti-tumor immune responses have been demonstrated post-radiation in both murine models and occasional patients, supporting the hypothesis that the irradiated tumor can become an in situ vaccine. It is in this role, that radiation can be applied to induce anti-tumor T cells in lymphocyte-poor tumors, and possibly benefit patients who would otherwise fail to respond to immune checkpoint inhibitors. This review summarizes preclinical and clinical data demonstrating that radiation acts in concert with antibodies targeting the immune checkpoint cytotoxic T-lymphocyte antigen-4 (CTLA-4), to induce therapeutically effective anti-tumor T cell responses in tumors otherwise non responsive to anti-CTLA-4 therapy.
Keywords: Abscopal effect; Immmune checkpoint; Immunotherapy; Radiation-induced vaccination.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Figures
References
-
- Vesely MD, Kershaw MH, Schreiber RD, Smyth MJ. Natural innate and adaptive immunity to cancer. Annu Rev Immunol. 2011;29:235–71. - PubMed
-
- Galon J, Costes A, Sanchez-Cabo F, Kirilovsky A, Mlecnik B, Lagorce-Pages C, et al. Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. Science. 2006;313:1960–4. - PubMed
-
- Pagès F, Galon J, Dieu-Nosjean MC, Tartour E, Sautès-Fridman C, Fridman WH. Immune infiltration in human tumors: a prognostic factor that should not be ignored. Oncogene. 2010;29:1093–102. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
