

Microcirculatory dysfunction and tissue oxygenation in critical illness
- PMID: 26149711
- PMCID: PMC4758388
- DOI: 10.1111/aas.12581
Microcirculatory dysfunction and tissue oxygenation in critical illness
Abstract
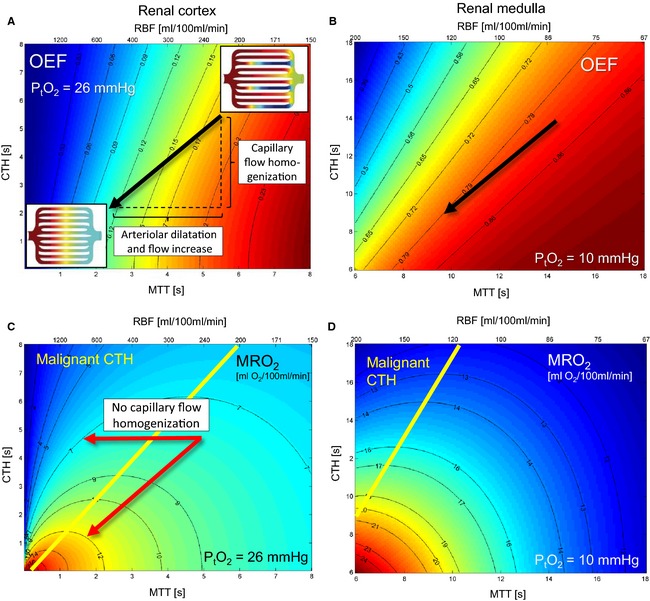
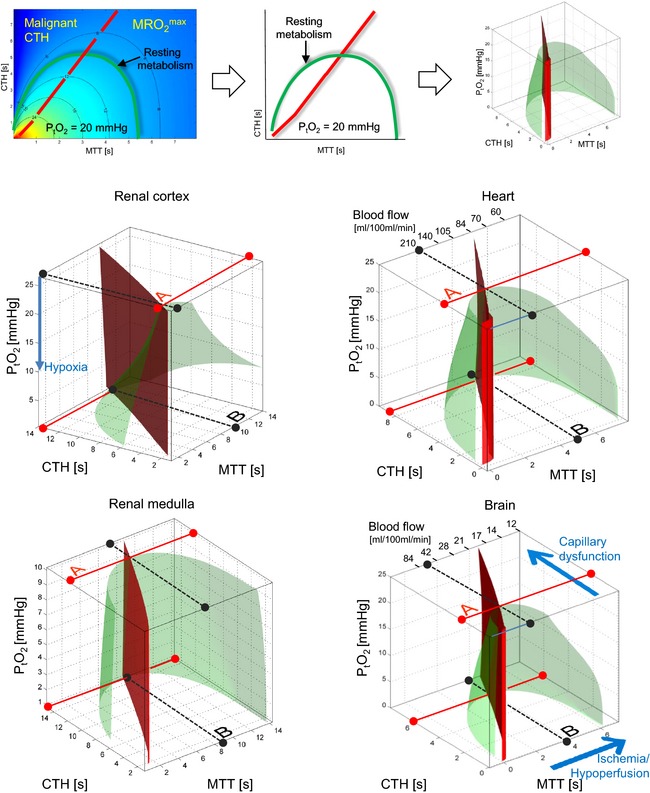
Severe sepsis is defined by organ failure, often of the kidneys, heart, and brain. It has been proposed that inadequate delivery of oxygen, or insufficient extraction of oxygen in tissue, may explain organ failure. Despite adequate maintenance of systemic oxygen delivery in septic patients, their morbidity and mortality remain high. The assumption that tissue oxygenation can be preserved by maintaining its blood supply follows from physiological models that only apply to tissue with uniformly perfused capillaries. In sepsis, the microcirculation is profoundly disturbed, and the blood supply of individual organs may therefore no longer reflect their access to oxygen. We review how capillary flow patterns affect oxygen extraction efficacy in tissue, and how the regulation of tissue blood flow must be adjusted to meet the metabolic needs of the tissue as capillary flows become disturbed as observed in critical illness. Using the brain, heart, and kidney as examples, we discuss whether disturbed capillary flow patterns might explain the apparent mismatch between organ blood flow and organ function in sepsis. Finally, we discuss diagnostic means of detecting capillary flow disturbance in animal models and in critically ill patients, and address therapeutic strategies that might improve tissue oxygenation by modifying capillary flow patterns.
© 2015 The Authors. Acta Anaesthesiologica Scandinavica published by John Wiley & Sons Ltd on behalf of Acta Anaesthesiologica Scandinavica Foundation.
Figures

References
-
- Hotchkiss RS, Karl IE. The pathophysiology and treatment of sepsis. N Engl J Med 2003; 348: 138–50. - PubMed
-
- Parker MM, Shelhamer JH, Natanson C, Alling DW, Parrillo JE. Serial cardiovascular variables in survivors and nonsurvivors of human septic shock: heart rate as an early predictor of prognosis. Crit Care Med 1987; 15: 923–9. - PubMed
-
- Kreymann G, Grosser S, Buggisch P, Gottschall C, Matthaei S, Greten H. Oxygen consumption and resting metabolic rate in sepsis, sepsis syndrome, and septic shock. Crit Care Med 1993; 21: 1012–9. - PubMed
-
- Hayes MA, Timmins AC, Yau EH, Palazzo M, Hinds CJ, Watson D. Elevation of systemic oxygen delivery in the treatment of critically ill patients. N Engl J Med 1994; 330: 1717–22. - PubMed
-
- Wan L, Bagshaw SM, Langenberg C, Saotome T, May C, Bellomo R. Pathophysiology of septic acute kidney injury: what do we really know? Crit Care Med 2008; 36: S198–203. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
