

Repeated nebulisation of non-viral CFTR gene therapy in patients with cystic fibrosis: a randomised, double-blind, placebo-controlled, phase 2b trial
- PMID: 26149841
- PMCID: PMC4673100
- DOI: 10.1016/S2213-2600(15)00245-3
Repeated nebulisation of non-viral CFTR gene therapy in patients with cystic fibrosis: a randomised, double-blind, placebo-controlled, phase 2b trial
Erratum in
-
Corrections.Lancet Respir Med. 2015 Sep;3(9):e33. doi: 10.1016/S2213-2600(15)00314-8. Epub 2015 Sep 6. Lancet Respir Med. 2015. PMID: 26380890 Free PMC article. No abstract available.
Abstract
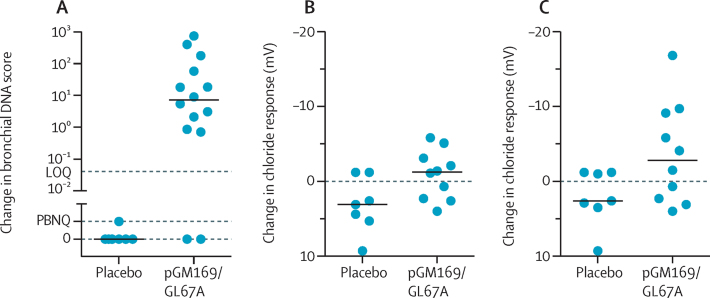
Background: Lung delivery of plasmid DNA encoding the CFTR gene complexed with a cationic liposome is a potential treatment option for patients with cystic fibrosis. We aimed to assess the efficacy of non-viral CFTR gene therapy in patients with cystic fibrosis.
Methods: We did this randomised, double-blind, placebo-controlled, phase 2b trial in two cystic fibrosis centres with patients recruited from 18 sites in the UK. Patients (aged ≥12 years) with a forced expiratory volume in 1 s (FEV1) of 50-90% predicted and any combination of CFTR mutations, were randomly assigned, via a computer-based randomisation system, to receive 5 mL of either nebulised pGM169/GL67A gene-liposome complex or 0.9% saline (placebo) every 28 days (plus or minus 5 days) for 1 year. Randomisation was stratified by % predicted FEV1 (<70 vs ≥70%), age (<18 vs ≥18 years), inclusion in the mechanistic substudy, and dosing site (London or Edinburgh). Participants and investigators were masked to treatment allocation. The primary endpoint was the relative change in % predicted FEV1. The primary analysis was per protocol. This trial is registered with ClinicalTrials.gov, number NCT01621867.
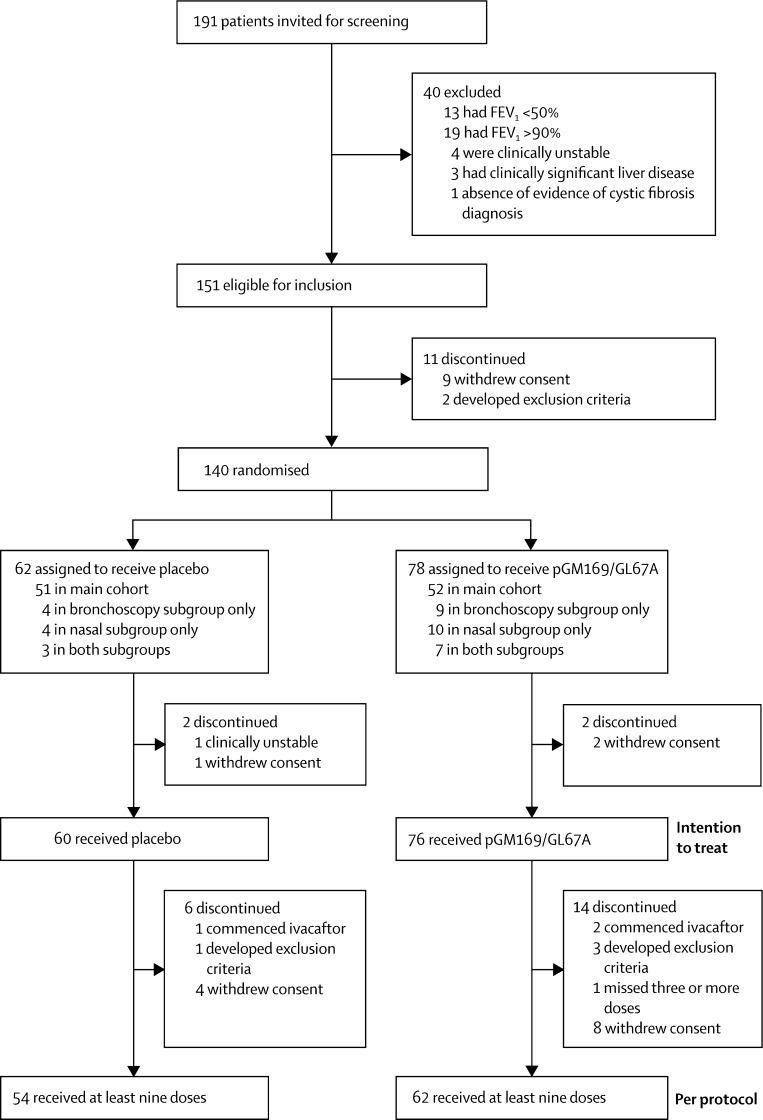
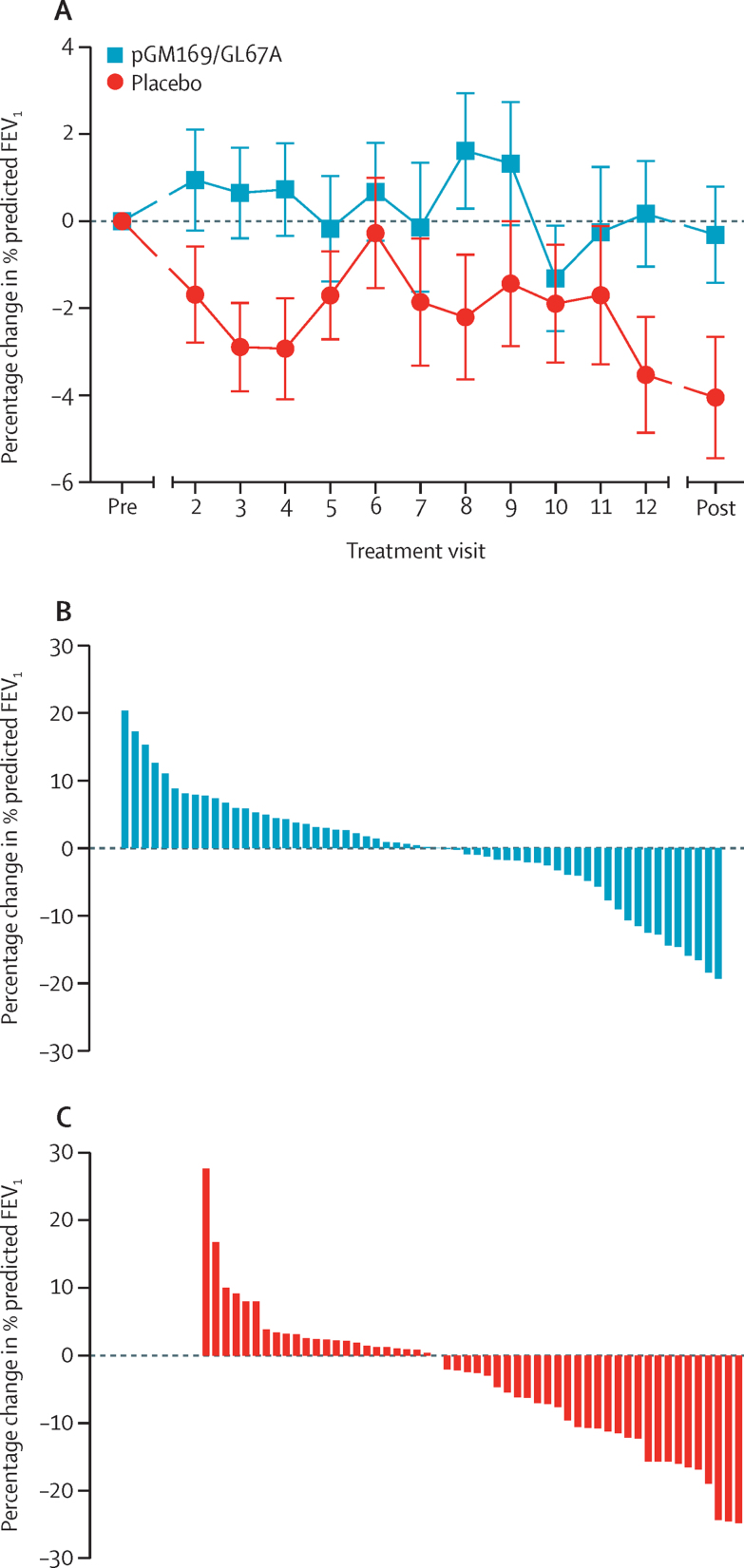
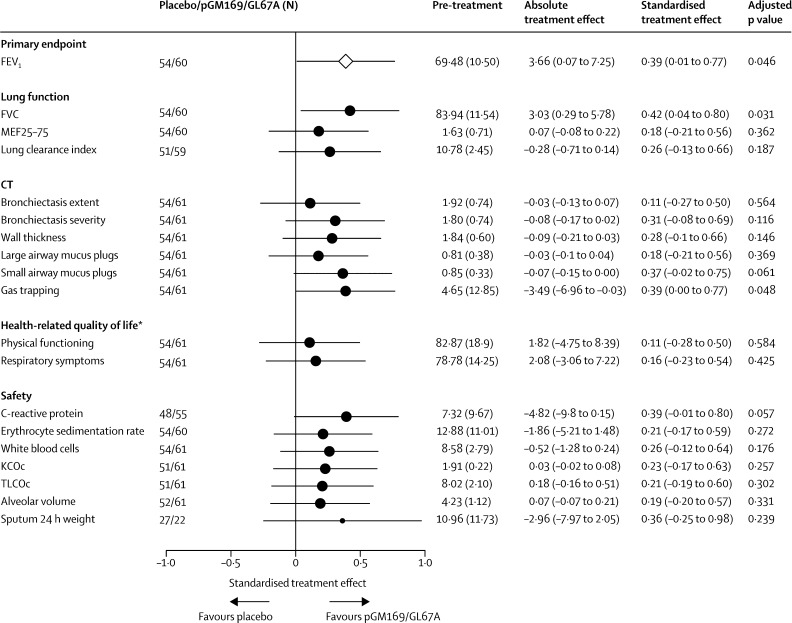
Findings: Between June 12, 2012, and June 24, 2013, we randomly assigned 140 patients to receive placebo (n=62) or pGM169/GL67A (n=78), of whom 116 (83%) patients comprised the per-protocol population. We noted a significant, albeit modest, treatment effect in the pGM169/GL67A group versus placebo at 12 months' follow-up (3.7%, 95% CI 0.1-7.3; p=0.046). This outcome was associated with a stabilisation of lung function in the pGM169/GL67A group compared with a decline in the placebo group. We recorded no significant difference in treatment-attributable adverse events between groups.
Interpretation: Monthly application of the pGM169/GL67A gene therapy formulation was associated with a significant, albeit modest, benefit in FEV1 compared with placebo at 1 year, indicating a stabilisation of lung function in the treatment group. Further improvements in efficacy and consistency of response to the current formulation are needed before gene therapy is suitable for clinical care; however, our findings should also encourage the rapid introduction of more potent gene transfer vectors into early phase trials.
Funding: Medical Research Council/National Institute for Health Research Efficacy and Mechanism Evaluation Programme.
Copyright © 2015 Alton et al. Open Access article distributed under the terms of CC BY. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
A new phase of CFTR treatment for cystic fibrosis?Lancet Respir Med. 2015 Sep;3(9):662-663. doi: 10.1016/S2213-2600(15)00282-9. Epub 2015 Jul 22. Lancet Respir Med. 2015. PMID: 26208999 No abstract available.
References
-
- Griesenbach U, Alton EW. Moving forward: cystic fibrosis gene therapy. Hum Mol Genet. 2013;22:R52–R58. - PubMed
-
- Cystic Fibrosis Trust UK Cystic Fibrosis Registry annual data report 2013. 2014. http://www.cysticfibrosis.org.uk/media/598466/annual-data-report-2013-ju... (accessed April 26, 2015).
-
- Gill DR, Hyde SC. Delivery of genes into the CF airway. Thorax. 2014;69:962–964. - PubMed
-
- Davies LA, Nunez-Alonso GA, McLachlan G, Hyde SC, Gill DR. Aerosol delivery of DNA/liposomes to the lung for cystic fibrosis gene therapy. Hum Gene Ther Clin Dev. 2014;25:97–107. - PubMed
-
- McLachlan G, Davidson H, Holder E. Pre-clinical evaluation of three non-viral gene transfer agents for cystic fibrosis after aerosol delivery to the ovine lung. Gene Ther. 2011;18:996–1005. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
