

Success of Anomia Treatment in Aphasia Is Associated With Preserved Architecture of Global and Left Temporal Lobe Structural Networks
- PMID: 26150147
- PMCID: PMC4703576
- DOI: 10.1177/1545968315593808
Success of Anomia Treatment in Aphasia Is Associated With Preserved Architecture of Global and Left Temporal Lobe Structural Networks
Abstract
Background and objective: Targeted speech therapy can lead to substantial naming improvement in some subjects with anomia following dominant-hemisphere stroke. We investigated whether treatment-induced improvement in naming is associated with poststroke preservation of structural neural network architecture.
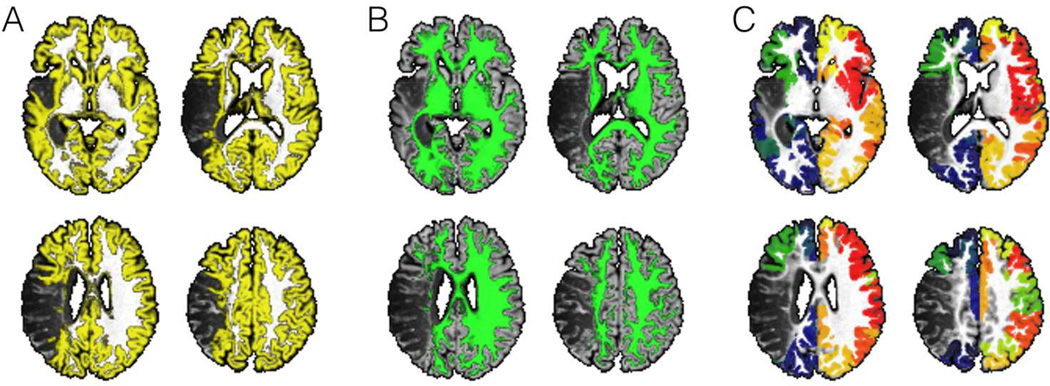
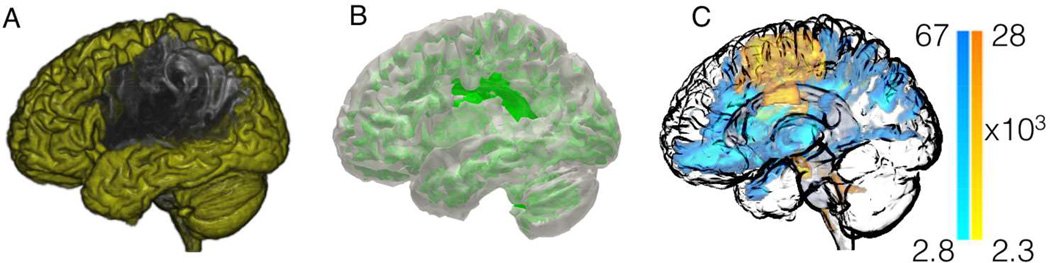
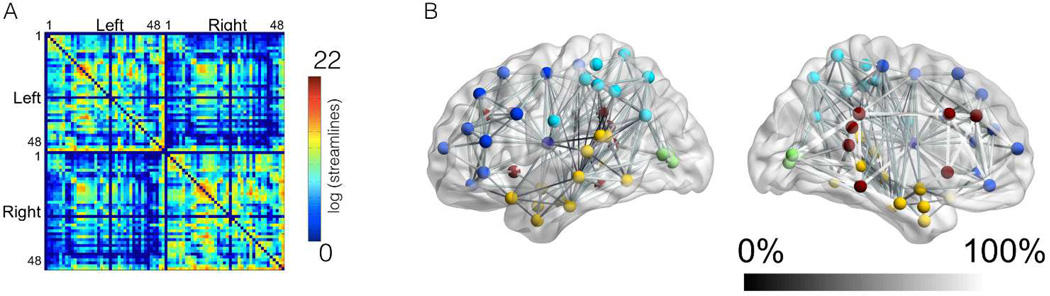
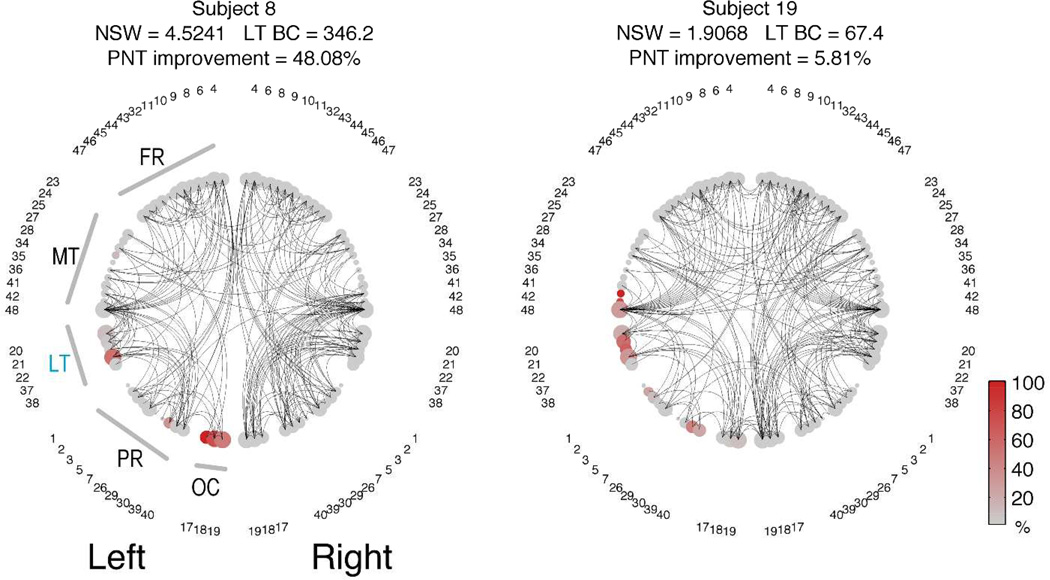
Methods: Twenty-four patients with poststroke chronic aphasia underwent 30 hours of speech therapy over a 2-week period and were assessed at baseline and after therapy. Whole brain maps of neural architecture were constructed from pretreatment diffusion tensor magnetic resonance imaging to derive measures of global brain network architecture (network small-worldness) and regional network influence (nodal betweenness centrality). Their relationship with naming recovery was evaluated with multiple linear regressions.
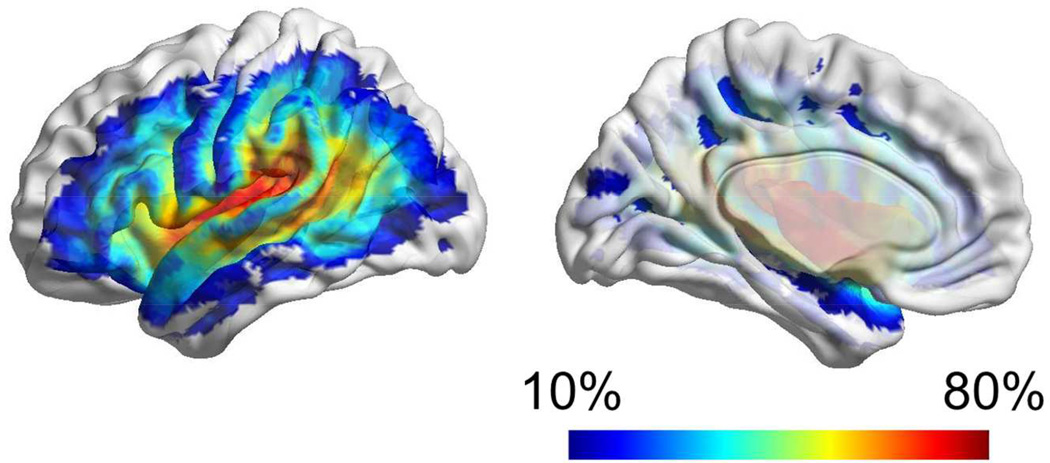
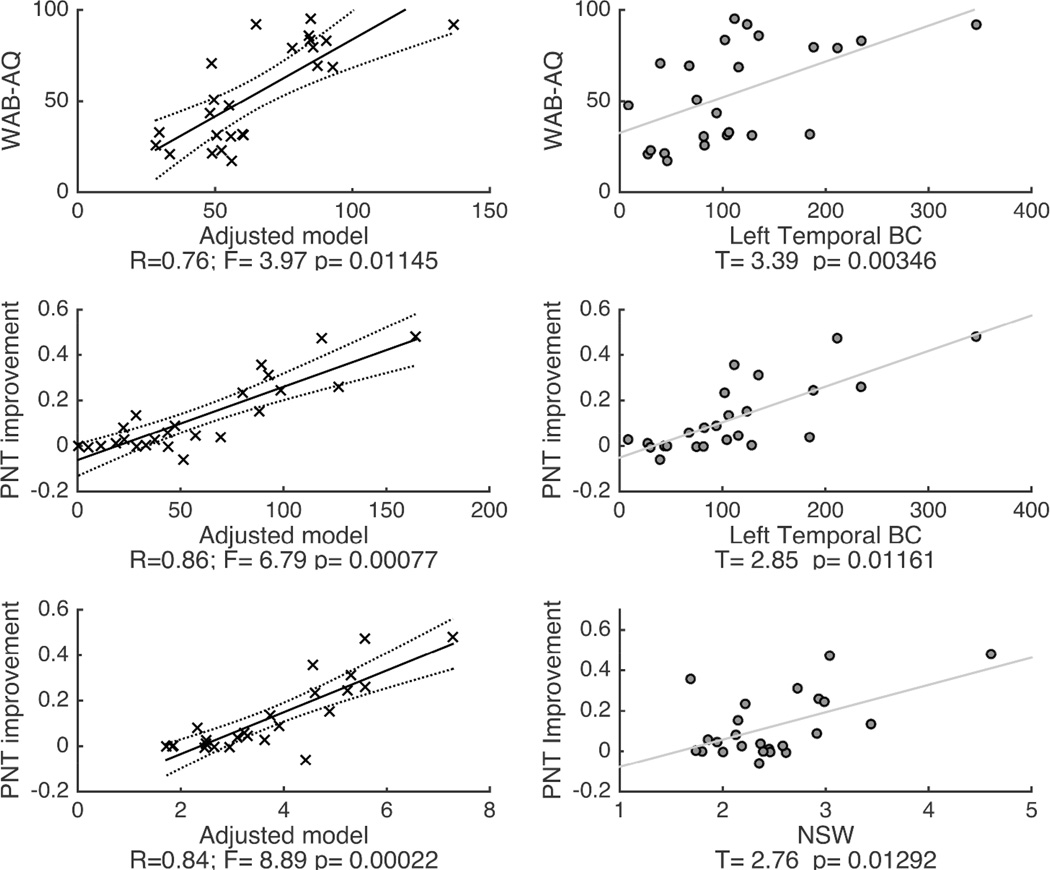
Results: Treatment-induced improvement in correct naming was associated with poststroke preservation of global network small worldness and of betweenness centrality in temporal lobe cortical regions. Together with baseline aphasia severity, these measures explained 78% of the variability in treatment response.
Conclusions: Preservation of global and left temporal structural connectivity broadly explains the variability in treatment-related naming improvement in aphasia. These findings corroborate and expand on previous classical lesion-symptom mapping studies by elucidating some of the mechanisms by which brain damage may relate to treated aphasia recovery. Favorable naming outcomes may result from the intact connections between spared cortical areas that are functionally responsive to treatment.
Keywords: aphasia; diffusion tensor imaging; magnetic resonance imaging; naming; recovery; structural connectome.
© The Author(s) 2015.
Figures
References
-
- Donnan GA, Fisher M, Macleod M, Davis SM. Stroke. Lancet. 2008 May 10;371(9624):1612–1623. - PubMed
-
- Croquelois A, Bogousslavsky J. Stroke aphasia: 1,500 consecutive cases. Cerebrovascular diseases. 2011;31(4):392–399. - PubMed
-
- Hilari K, Byng S. Health-related quality of life in people with severe aphasia. International journal of language & communication disorders / Royal College of Speech & Language Therapists. 2009 Mar-Apr;44(2):193–205. - PubMed
-
- Kohn SE, Goodglass H. Picture-naming in aphasia. Brain and language. 1985 Mar;24(2):266–283. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
