

Race and Insurance Differences in the Receipt of Adjuvant Chemotherapy Among Patients With Stage III Colon Cancer
- PMID: 26150445
- PMCID: PMC4525047
- DOI: 10.1200/JCO.2015.61.3026
Race and Insurance Differences in the Receipt of Adjuvant Chemotherapy Among Patients With Stage III Colon Cancer
Abstract
Purpose: Although the incidence and mortality of colon cancer in the United States has declined over the past two decades, blacks have worse outcomes than whites. Variations in treatment may contribute to mortality differentials.
Methods: Patients diagnosed with stage III colon cancer were randomly sampled from the SEER program from the years 1990, 1991, 1995, 2000, 2005, and 2010. Patients were categorized as non-Hispanic white (n = 835) or black (n = 384). Treatment data were obtained from a review of the medical records, and these data were verified through contact with the original treating physicians. Log-binomial regression models were used to estimate the association between race and receipt of adjuvant chemotherapy. Effect modification by insurance was assessed with use of single referent models.
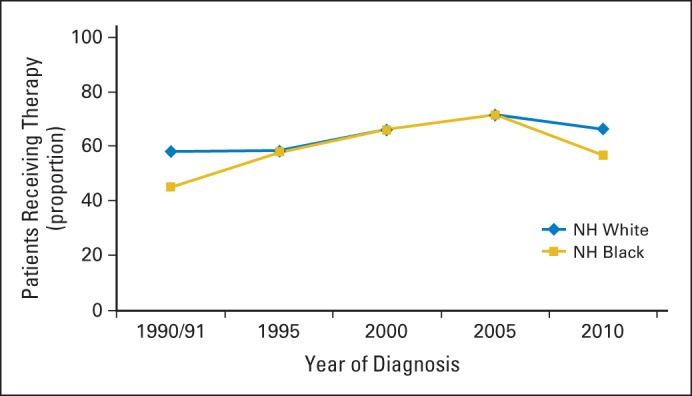
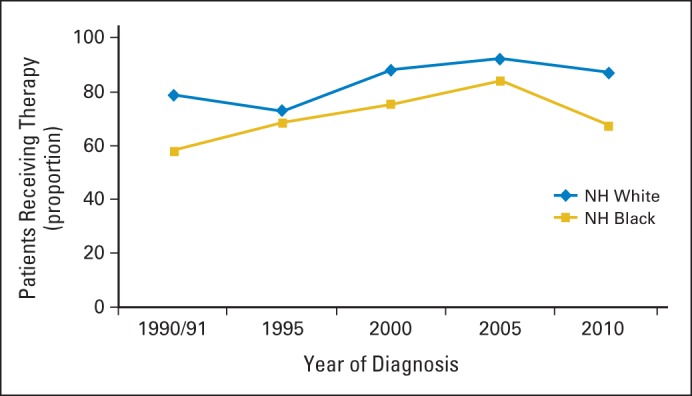
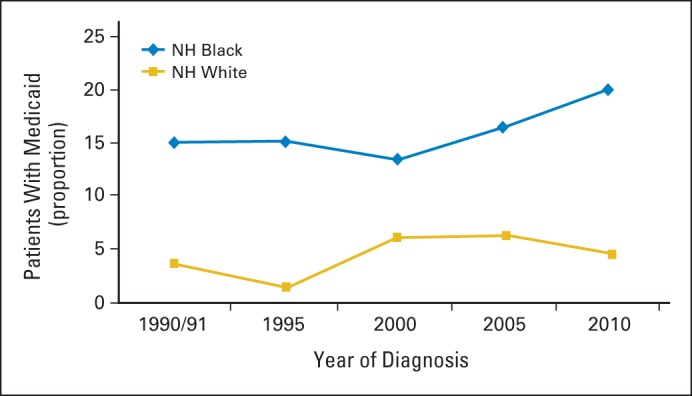
Results: Receipt of adjuvant chemotherapy among both white and black patients increased from the period encompassing the years 1990 and 1991 (white, 58%; black, 45%) to the year 2005 (white, 72%; black, 71%) and then decreased in the year 2010 (white, 66%; black, 57%). There were marked racial disparities in the time period of 1990 to 1991 and again in 2010, with black patients less likely to receive adjuvant chemotherapy as compared with white patients (risk ratio [RR], .82; 95% CI, .72 to .93). For black patients, receipt of adjuvant chemotherapy did not differ across insurance categories (RR for private insurance, .80; 95% CI, .69 to .93; RR for Medicare, .84; 95% CI, .69 to 1.02; and RR for Medicaid, .84; 95% CI, .69 to 1.02), although a larger proportion had Medicaid in all years of the study as compared with white patients.
Conclusion: The chemotherapy differential narrowed after the time period of 1990 to 1991, but our findings suggest that the disparity reemerged in 2010. Recent decreases in chemotherapy use may be due, in part, to the economic downturn and an increase in Medicaid coverage.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures
References
-
- National Cancer Institute. surveillance, epidemiology, and end results. Cancer Statistics Review. 2013:1975–2011.
-
- Siegel R, Desantis C, Jemal A. Colorectal cancer statistics, 2014. CA Cancer J Clin. 2014;64:104–117. - PubMed
-
- Robbins AS, Siegel RL, Jemal A. Racial disparities in stage-specific colorectal cancer mortality rates from 1985 to 2008. J Clin Oncol. 2012;30:401–405. - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN261201000140C/CA/NCI NIH HHS/United States
- HHSN261201000032C/CA/NCI NIH HHS/United States
- T32 DK07634/DK/NIDDK NIH HHS/United States
- HHSN261201000031C/CA/NCI NIH HHS/United States
- HHSN261201000035I/CA/NCI NIH HHS/United States
- HHSN261201000029C/CA/NCI NIH HHS/United States
- HHSN261201000026C/CA/NCI NIH HHS/United States
- HHSN261201000037C/CA/NCI NIH HHS/United States
- HHSN261201000027C/CA/NCI NIH HHS/United States
- HHSN261201000024C/CA/NCI NIH HHS/United States
- HHSN261201000035C/PC/NCI NIH HHS/United States
- HHSN261201000030C/CA/NCI NIH HHS/United States
- HHSN261201000033C/CA/NCI NIH HHS/United States
- T32 DK007634/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
