

The PROPKD Score: A New Algorithm to Predict Renal Survival in Autosomal Dominant Polycystic Kidney Disease
- PMID: 26150605
- PMCID: PMC4769200
- DOI: 10.1681/ASN.2015010016
The PROPKD Score: A New Algorithm to Predict Renal Survival in Autosomal Dominant Polycystic Kidney Disease
Abstract
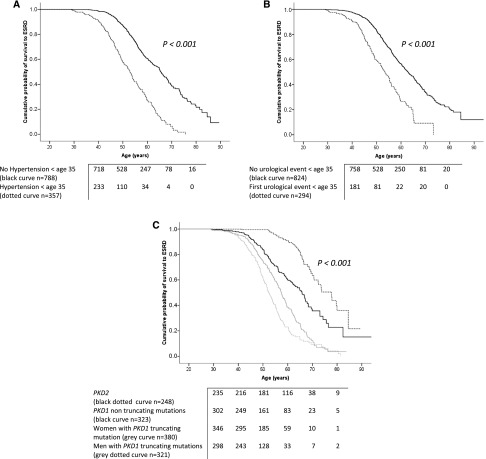
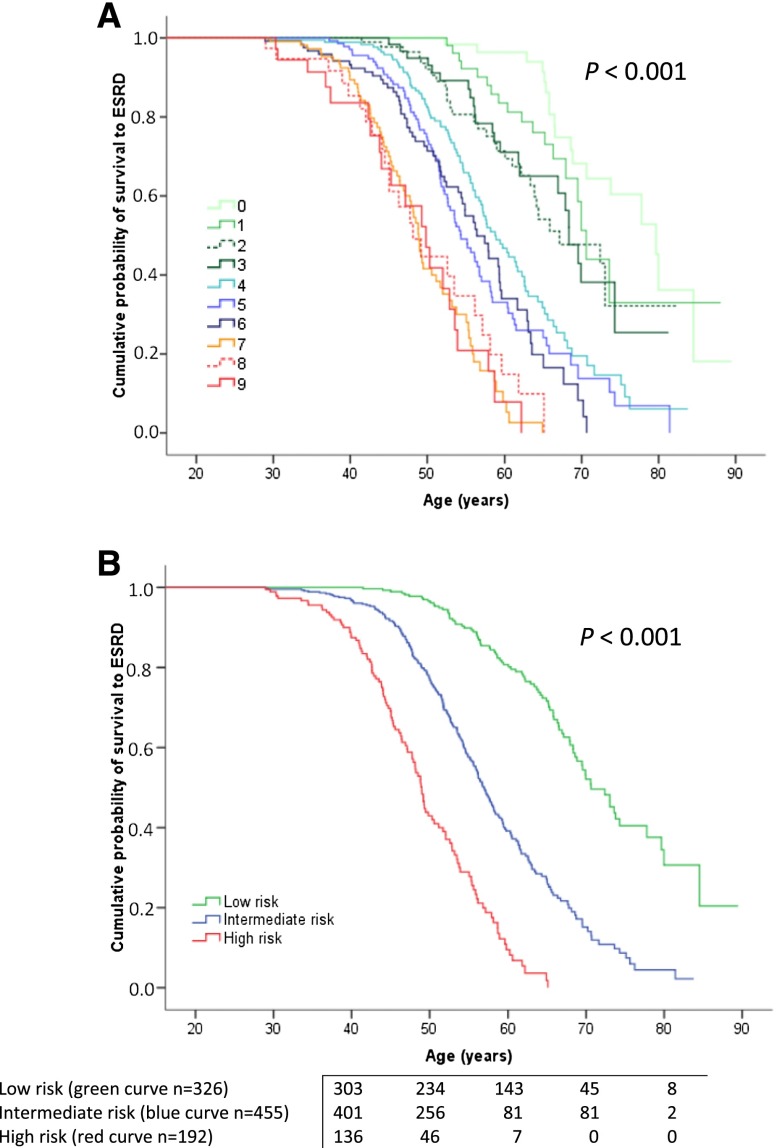
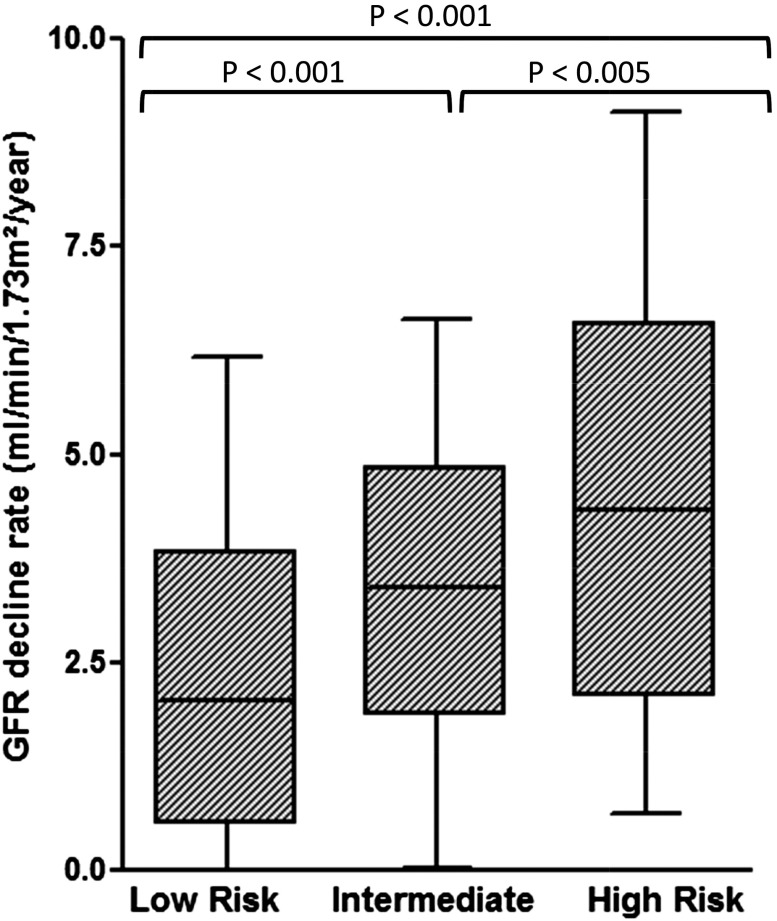
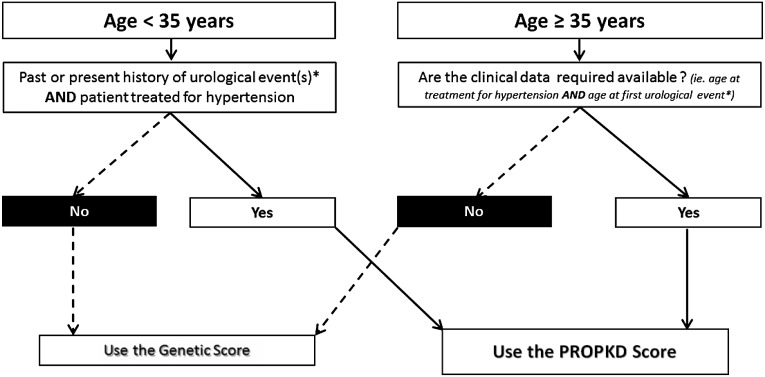
The course of autosomal dominant polycystic kidney disease (ADPKD) varies among individuals, with some reaching ESRD before 40 years of age and others never requiring RRT. In this study, we developed a prognostic model to predict renal outcomes in patients with ADPKD on the basis of genetic and clinical data. We conducted a cross-sectional study of 1341 patients from the Genkyst cohort and evaluated the influence of clinical and genetic factors on renal survival. Multivariate survival analysis identified four variables that were significantly associated with age at ESRD onset, and a scoring system from 0 to 9 was developed as follows: being male: 1 point; hypertension before 35 years of age: 2 points; first urologic event before 35 years of age: 2 points; PKD2 mutation: 0 points; nontruncating PKD1 mutation: 2 points; and truncating PKD1 mutation: 4 points. Three risk categories were subsequently defined as low risk (0-3 points), intermediate risk (4-6 points), and high risk (7-9 points) of progression to ESRD, with corresponding median ages for ESRD onset of 70.6, 56.9, and 49 years, respectively. Whereas a score ≤3 eliminates evolution to ESRD before 60 years of age with a negative predictive value of 81.4%, a score >6 forecasts ESRD onset before 60 years of age with a positive predictive value of 90.9%. This new prognostic score accurately predicts renal outcomes in patients with ADPKD and may enable the personalization of therapeutic management of ADPKD.
Keywords: ADPKD; end-stage renal disease; genetic renal disease; progression of renal failure; risk factors.
Copyright © 2016 by the American Society of Nephrology.
Figures
References
-
- Torres VE, Harris PC, Pirson Y: Autosomal dominant polycystic kidney disease. Lancet 369: 1287–1301, 2007 - PubMed
-
- Shaw C, Simms RJ, Pitcher D, Sandford R: Epidemiology of patients in England and Wales with autosomal dominant polycystic kidney disease and end-stage renal failure. Nephrol Dial Transplant 29: 1910–1918, 2014 - PubMed
-
- Cornec-Le Gall E, Audrézet M-P, Meur YL, Chen J-M, Férec C: Genetics and pathogenesis of autosomal dominant polycystic kidney disease: 20 years on. Hum Mutat 35: 1393–1406, 2014 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
