

Gut-liver axis, nutrition, and non-alcoholic fatty liver disease
- PMID: 26151226
- PMCID: PMC4558208
- DOI: 10.1016/j.clinbiochem.2015.06.023
Gut-liver axis, nutrition, and non-alcoholic fatty liver disease
Abstract
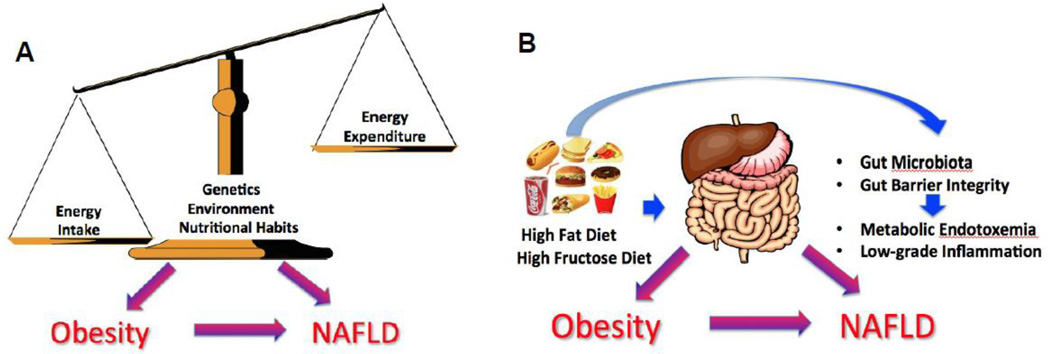
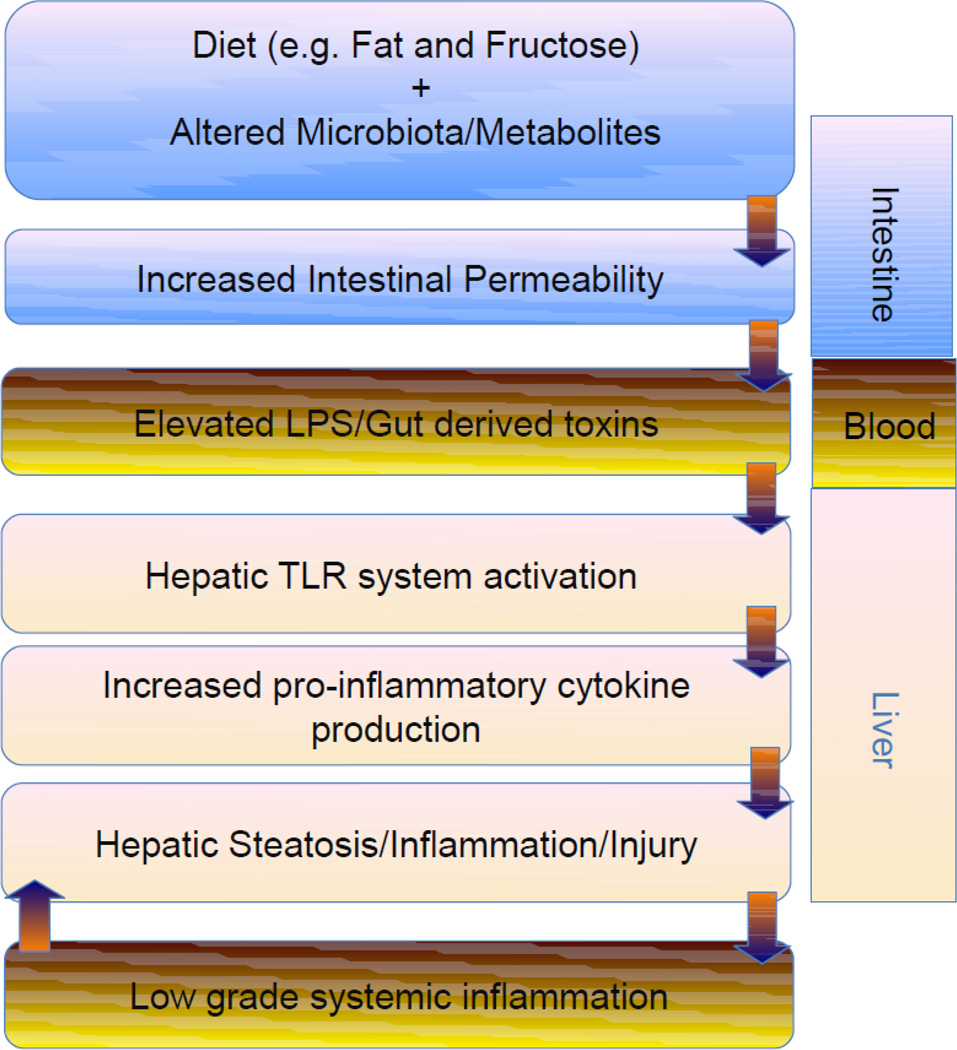
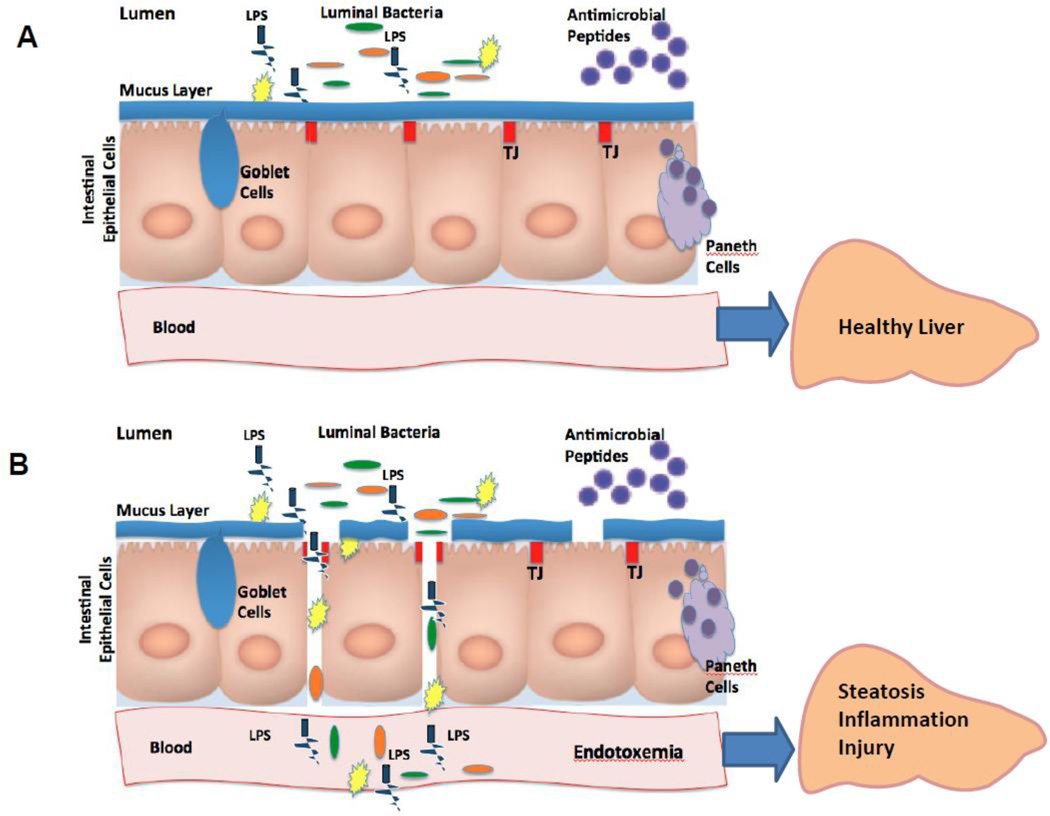
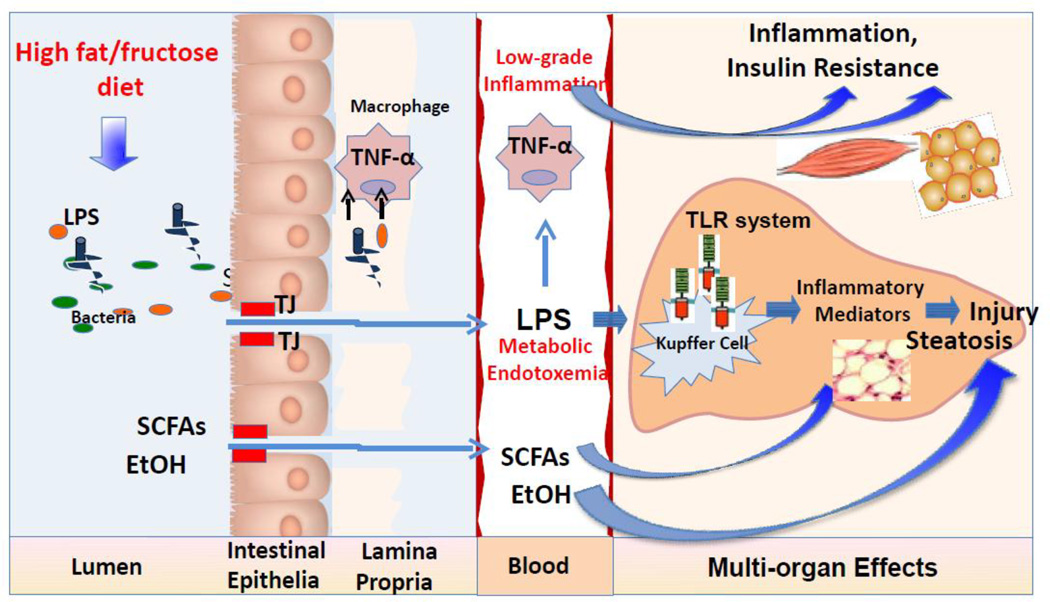
Nonalcoholic fatty liver disease (NAFLD) represents a spectrum of diseases involving hepatic fat accumulation, inflammation with the potential progression to fibrosis and cirrhosis over time. NAFLD is often associated with obesity, insulin resistance, and diabetes. The interactions between the liver and the gut, the so-called "gut-liver axis", play a critical role in NAFLD onset and progression. Compelling evidence links the gut microbiome, intestinal barrier integrity, and NAFLD. The dietary factors may alter the gut microbiota and intestinal barrier function, favoring the occurrence of metabolic endotoxemia and low grade inflammation, thereby contributing to the development of obesity and obesity-associated fatty liver disease. Therapeutic manipulations with prebiotics and probiotics to modulate the gut microbiota and maintain intestinal barrier integrity are potential agents for NAFLD management. This review summarizes the current knowledge regarding the complex interplay between the gut microbiota, intestinal barrier, and dietary factors in NAFLD pathogenesis. The concepts addressed in this review have important clinical implications, although more work needs to be done to understand how dietary factors affect the gut barrier and microbiota, and to comprehend how microbe-derived components may interfere with the host's metabolism contributing to NAFLD development.
Keywords: Dietary factors; Gut microbiome; Intestinal barrier; Metabolic endotoxemia; Nonalcoholic fatty liver disease.
Copyright © 2015 The Canadian Society of Clinical Chemists. All rights reserved.
Conflict of interest statement
Figures
References
-
- Sheth SG, Gordon FD, Chopra S. Nonalcoholic steatohepatitis. Ann Intern Med. 1997;126(2):137–145. - PubMed
-
- Browning JD, et al. Prevalence of hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology. 2004;40(6):1387–1395. - PubMed
-
- Kelly T, et al. Global burden of obesity in 2005 and projections to 2030. Int J Obes (Lond) 2008;32(9):1431–1437. - PubMed
-
- Cani PD, et al. Selective increases of bifidobacteria in gut microflora improve high-fat-diet-induced diabetes in mice through a mechanism associated with endotoxaemia. Diabetologia. 2007;50(11):2374–2383. - PubMed
-
- Cani PD, et al. Metabolic endotoxemia initiates obesity and insulin resistance. Diabetes. 2007;56(7):1761–1772. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
