

Association of Cardiometabolic Multimorbidity With Mortality
- PMID: 26151266
- PMCID: PMC4664176
- DOI: 10.1001/jama.2015.7008
Association of Cardiometabolic Multimorbidity With Mortality
Erratum in
-
Author's Middle Initials Missing in Byline.JAMA. 2015 Sep 15;314(11):1179. doi: 10.1001/jama.2015.10410. JAMA. 2015. PMID: 26372596 No abstract available.
Abstract
Importance: The prevalence of cardiometabolic multimorbidity is increasing.
Objective: To estimate reductions in life expectancy associated with cardiometabolic multimorbidity.
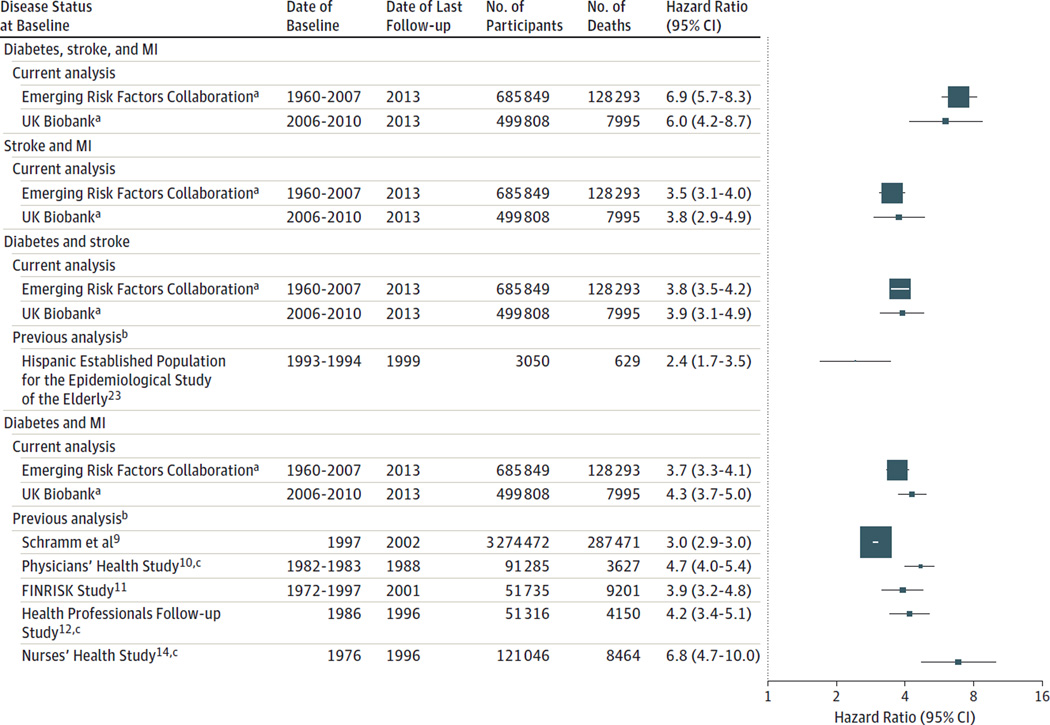
Design, setting, and participants: Age- and sex-adjusted mortality rates and hazard ratios (HRs) were calculated using individual participant data from the Emerging Risk Factors Collaboration (689,300 participants; 91 cohorts; years of baseline surveys: 1960-2007; latest mortality follow-up: April 2013; 128,843 deaths). The HRs from the Emerging Risk Factors Collaboration were compared with those from the UK Biobank (499,808 participants; years of baseline surveys: 2006-2010; latest mortality follow-up: November 2013; 7995 deaths). Cumulative survival was estimated by applying calculated age-specific HRs for mortality to contemporary US age-specific death rates.
Exposures: A history of 2 or more of the following: diabetes mellitus, stroke, myocardial infarction (MI).
Main outcomes and measures: All-cause mortality and estimated reductions in life expectancy.
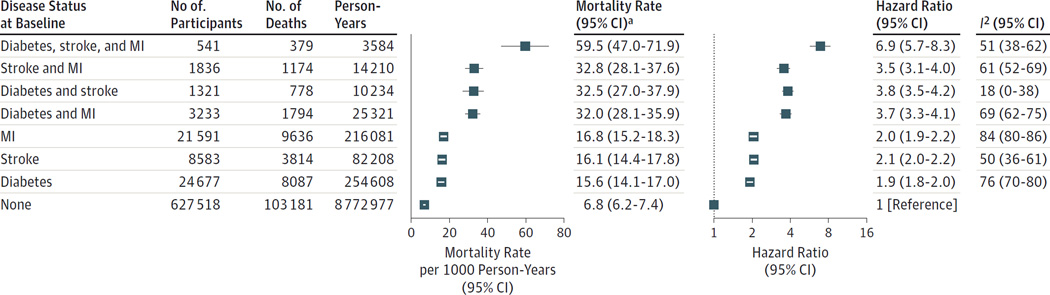
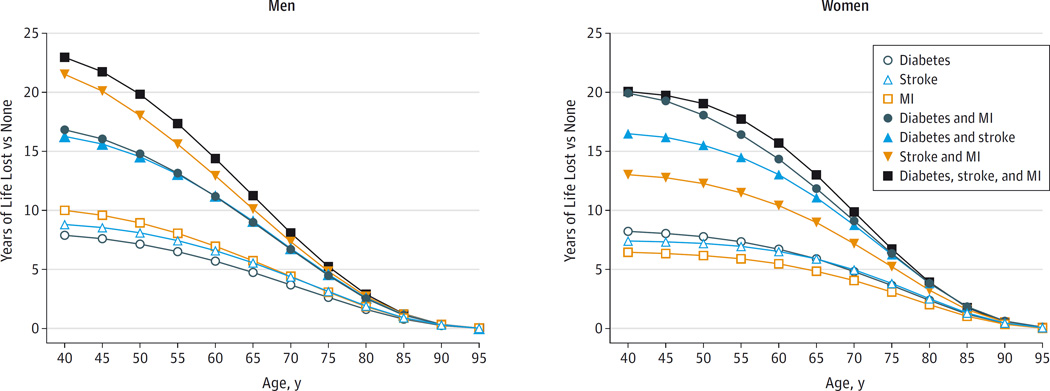
Results: In participants in the Emerging Risk Factors Collaboration without a history of diabetes, stroke, or MI at baseline (reference group), the all-cause mortality rate adjusted to the age of 60 years was 6.8 per 1000 person-years. Mortality rates per 1000 person-years were 15.6 in participants with a history of diabetes, 16.1 in those with stroke, 16.8 in those with MI, 32.0 in those with both diabetes and MI, 32.5 in those with both diabetes and stroke, 32.8 in those with both stroke and MI, and 59.5 in those with diabetes, stroke, and MI. Compared with the reference group, the HRs for all-cause mortality were 1.9 (95% CI, 1.8-2.0) in participants with a history of diabetes, 2.1 (95% CI, 2.0-2.2) in those with stroke, 2.0 (95% CI, 1.9-2.2) in those with MI, 3.7 (95% CI, 3.3-4.1) in those with both diabetes and MI, 3.8 (95% CI, 3.5-4.2) in those with both diabetes and stroke, 3.5 (95% CI, 3.1-4.0) in those with both stroke and MI, and 6.9 (95% CI, 5.7-8.3) in those with diabetes, stroke, and MI. The HRs from the Emerging Risk Factors Collaboration were similar to those from the more recently recruited UK Biobank. The HRs were little changed after further adjustment for markers of established intermediate pathways (eg, levels of lipids and blood pressure) and lifestyle factors (eg, smoking, diet). At the age of 60 years, a history of any 2 of these conditions was associated with 12 years of reduced life expectancy and a history of all 3 of these conditions was associated with 15 years of reduced life expectancy.
Conclusions and relevance: Mortality associated with a history of diabetes, stroke, or MI was similar for each condition. Because any combination of these conditions was associated with multiplicative mortality risk, life expectancy was substantially lower in people with multimorbidity.
Conflict of interest statement
Figures
References
-
- Glynn LG. Multimorbidity: another key issue for cardiovascular medicine. Lancet. 2009;374(9699):1421–1422. - PubMed
-
- Weiss CO, Boyd CM, Yu Q, et al. Patterns of prevalent major chronic disease among older adults in the United States. JAMA. 2007;298(10):1160–1162. - PubMed
-
- Booth GL, Kapral MK, Fung K, Tu JV. Relation between age and cardiovascular disease in men and women with diabetes compared with non-diabetic people. Lancet. 2006;368(9529):29–36. - PubMed
Publication types
MeSH terms
Grants and funding
- MC_U147585827/MRC_/Medical Research Council/United Kingdom
- P30 ES005605/ES/NIEHS NIH HHS/United States
- MC_QA137853/MRC_/Medical Research Council/United Kingdom
- RG/08/014/24067/BHF_/British Heart Foundation/United Kingdom
- MR/L003120/1/MRC_/Medical Research Council/United Kingdom
- MC_U106179471/MRC_/Medical Research Council/United Kingdom
- UL1 TR000062/TR/NCATS NIH HHS/United States
- G0401527/MRC_/Medical Research Council/United Kingdom
- 268834/ERC_/European Research Council/International
- G0701619/MRC_/Medical Research Council/United Kingdom
- MC_UU_12011/1/MRC_/Medical Research Council/United Kingdom
- G0700463/MRC_/Medical Research Council/United Kingdom
- G0400491/MRC_/Medical Research Council/United Kingdom
- MC_U147585819/MRC_/Medical Research Council/United Kingdom
- G1000143/MRC_/Medical Research Council/United Kingdom
- MC_UU_12015/1/MRC_/Medical Research Council/United Kingdom
- MC_UP_A620_1014/MRC_/Medical Research Council/United Kingdom
- MC_PC_12028/MRC_/Medical Research Council/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- MC_U147585824/MRC_/Medical Research Council/United Kingdom
- UL1 TR001450/TR/NCATS NIH HHS/United States
- SP/09/002/BHF_/British Heart Foundation/United Kingdom
- G0800270/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
