

Trends in Prevalence of HIV-1 Drug Resistance in a Public Clinic in Maputo, Mozambique
- PMID: 26151752
- PMCID: PMC4494809
- DOI: 10.1371/journal.pone.0130580
Trends in Prevalence of HIV-1 Drug Resistance in a Public Clinic in Maputo, Mozambique
Abstract
Background: An observational study was conducted in Maputo, Mozambique, to investigate trends in prevalence of HIV drug resistance (HIVDR) in antiretroviral (ART) naïve subjects initiating highly active antiretroviral treatment (HAART).
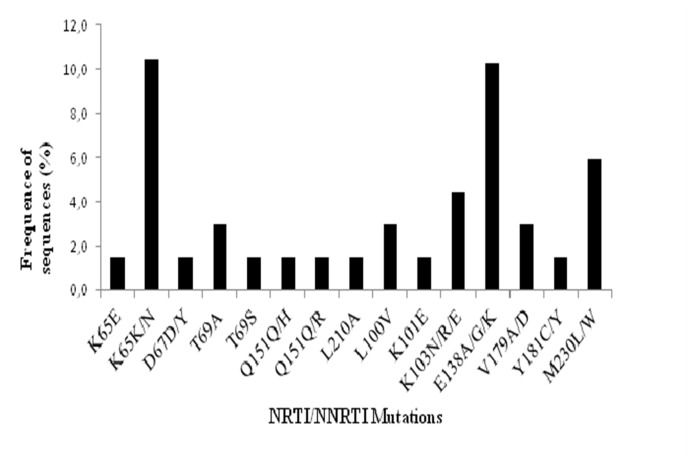
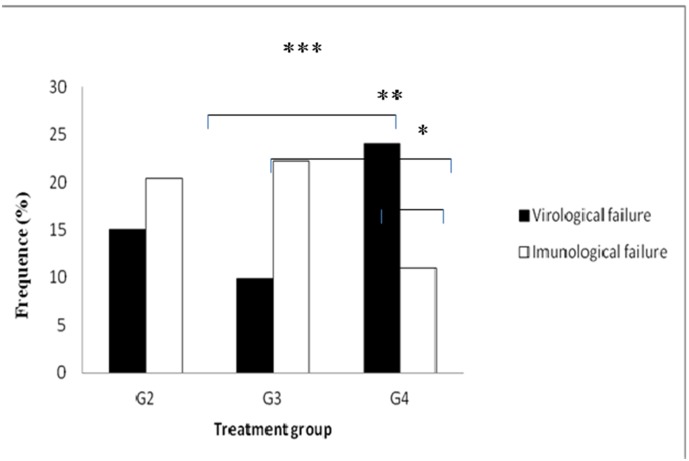
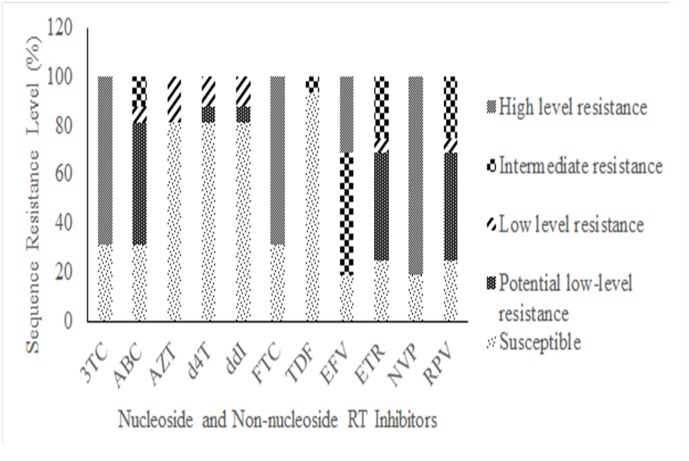
Methodology/principal findings: To evaluate the pattern of drug resistance mutations (DRMs) found in adults on ART failing first-line HAART [patients with detectable viral load (VL)]. Untreated subjects [Group 1 (G1; n=99)] and 274 treated subjects with variable length of exposure to ARV´s [6-12 months, Group 2 (G2;n=93); 12-24 months, Group 3 (G3;n=81); >24 months (G4;n=100)] were enrolled. Virological and immunological failure (VF and IF) were measured based on viral load (VL) and T lymphocyte CD4+ cells (TCD4+) count and genotypic resistance was also performed. Major subtype found was C (untreated: n=66, 97,06%; treated: n=36, 91.7%). Maximum virological suppression was observed in G3, and significant differences intragroup were observed between VF and IF in G4 (p=0.022). Intergroup differences were observed between G3 and G4 for VF (p=0.023) and IF between G2 and G4 (p=0.0018). Viral suppression (<50 copies/ml) ranged from 84.9% to 90.1%, and concordant VL and DRM ranged from 25% to 57%. WHO cut-off for determining VF as given by 2010 guidelines (>5000 copies/ml) identified 50% of subjects carrying DRM compared to 100% when lower VL cut-off was used (<50 copies/ml). Length of exposure to ARVs was directly proportional to the complexity of DRM patterns. In Mozambique, VL suppression was achieved in 76% of individuals after 24 months on HAART. This is in agreement with WHO target for HIVDR prevention target (70%).
Conclusions: We demonstrated that the best way to determine therapeutic failure is VL compared to CD4 counts. The rationalized use of VL testing is needed to ensure timely detection of treatment failures preventing the occurrence of TDR and new infections.
Conflict of interest statement
Figures
Similar articles
-
HIV-1 drug resistance and associated factors among adults failing first-line highly active antiretroviral therapy in Ho Chi Minh City, Vietnam.HIV Clin Trials. 2013 Jan-Feb;14(1):34-44. doi: 10.1310/hct1401-34. HIV Clin Trials. 2013. PMID: 23372113
-
Study of the impact of HIV genotypic drug resistance testing on therapy efficacy.Verh K Acad Geneeskd Belg. 2001;63(5):447-73. Verh K Acad Geneeskd Belg. 2001. PMID: 11813503 Review.
-
Accumulation of HIV-1 drug resistance after continued virological failure on first-line ART in adults and children in sub-Saharan Africa.J Antimicrob Chemother. 2016 Oct;71(10):2918-27. doi: 10.1093/jac/dkw218. Epub 2016 Jun 23. J Antimicrob Chemother. 2016. PMID: 27342546
-
Low primary and secondary HIV drug-resistance after 12 months of antiretroviral therapy in human immune-deficiency virus type 1 (HIV-1)-infected individuals from Kigali, Rwanda.PLoS One. 2013 Aug 12;8(8):e64345. doi: 10.1371/journal.pone.0064345. eCollection 2013. PLoS One. 2013. PMID: 23950859 Free PMC article.
-
HIV-1 antiretroviral resistance: scientific principles and clinical applications.Drugs. 2012 Jun 18;72(9):e1-25. doi: 10.2165/11633630-000000000-00000. Drugs. 2012. PMID: 22686620 Free PMC article. Review.
Cited by
-
Association of HIV/AIDS Clinician Warm Line Utilization with Diagnosis and Management of Antiretroviral Treatment Failure in Mozambique: A Retrospective Analysis of Program Data.J Int Assoc Provid AIDS Care. 2017 Jul/Aug;16(4):396-404. doi: 10.1177/2325957417710720. Epub 2017 May 31. J Int Assoc Provid AIDS Care. 2017. PMID: 28560889 Free PMC article.
-
Molecular Epidemiology of HIV-1 Infected Migrants Followed up in Portugal: Trends between 2001-2017.Viruses. 2020 Feb 28;12(3):268. doi: 10.3390/v12030268. Viruses. 2020. PMID: 32121161 Free PMC article.
-
High rate of virological failure and low rate of switching to second-line treatment among adolescents and adults living with HIV on first-line ART in Myanmar, 2005-2015.PLoS One. 2017 Feb 9;12(2):e0171780. doi: 10.1371/journal.pone.0171780. eCollection 2017. PLoS One. 2017. PMID: 28182786 Free PMC article.
-
Journey towards universal viral load monitoring in Maputo, Mozambique: many gaps, but encouraging signs.Int Health. 2017 Jul 1;9(4):206-214. doi: 10.1093/inthealth/ihx021. Int Health. 2017. PMID: 28810670 Free PMC article.
-
The clinical outcome of HIV infection at a tertiary care center in Riyadh, Saudi Arabia.Saudi Med J. 2020 Sep;41(9):965-970. doi: 10.15537/smj.2020.9.25274. Saudi Med J. 2020. PMID: 32893278 Free PMC article.
References
-
- National Institute of Health NI of S (Mozambique) and C for DC (US). National Survey on Prevalence, Behavioral Risks and Information about HIV and AIDS (2009 INSIDA). 2009.
-
- Comité Nacional de Assistência Médica e Colaboradores. Guia de Tratamento Antiretroviral e Infecções Oportunistas no Adulto, Adolescente e Grávida.
-
- WHO. Antiretroviral therapy for HIV infection in adults and adolescents. Recommendations for a public health approach. 2010. - PubMed
-
- Mozambique Ministry of Health. Dados TARV Nacionais ate Dezembro 2012 Final. In: 2013 [Internet]. 2013. Available: http://www.misau.gov.mz/index.php/hiv-sida/cat_view/82-hivsida/89-inform...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
