

Proteinuria as a Noninvasive Marker for Renal Allograft Histology and Failure: An Observational Cohort Study
- PMID: 26152270
- PMCID: PMC4696583
- DOI: 10.1681/ASN.2015010062
Proteinuria as a Noninvasive Marker for Renal Allograft Histology and Failure: An Observational Cohort Study
Abstract
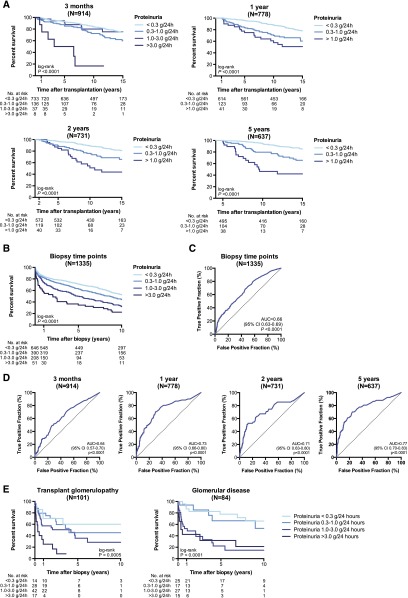
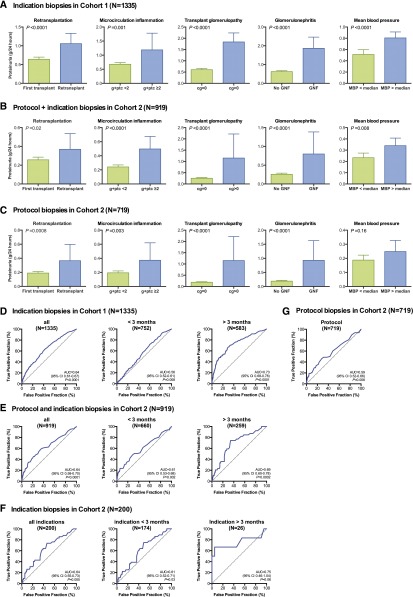
Proteinuria is routinely measured to assess renal allograft status, but the diagnostic and prognostic values of this measurement for renal transplant pathology and outcome remain unclear. We included 1518 renal allograft recipients in this prospective, observational cohort study. All renal allograft biopsy samples with concomitant data on 24-hour proteinuria were included in the analyses (n=2274). Patients were followed for ≥7 years post-transplantation. Compared with proteinuria <0.3 g/24 h, the hazard ratios for graft failure were 1.14 (95% confidence interval [95% CI], 0.81 to 1.60; P=0.50), for proteinuria 0.3-1.0 g/24 h, 2.17 (95% CI, 1.49 to 3.18; P<0.001), for proteinuria 1.0-3.0 g/24 h, and 3.01 (95% CI, 1.75 to 5.18; P<0.001), for proteinuria >3.0 g/24 h, independent of GFR and allograft histology. The predictive performance of proteinuria for graft failure was lower at 3 months after transplant (area under the receiver-operating characteristic curve [AUC] 0.64, P<0.001) than at 1, 2, and 5 years after transplant (AUC 0.73, 0.71, and 0.77, respectively, all P<0.001). Independent determinants of proteinuria were repeat transplantation, mean arterial pressure, transplant glomerulopathy, microcirculation inflammation, and de novo/recurrent glomerular disease. The discriminatory power of proteinuria for these intragraft injury processes was better in biopsy samples obtained >3 months after transplant (AUC 0.73, P<0.001) than in those obtained earlier (AUC 0.56, P<0.01), with 85% specificity but lower sensitivity (47.8%) for proteinuria >1.0 g/24 h. These data support current clinical guidelines to routinely measure proteinuria after transplant, but illustrate the need for more sensitive biomarkers of allograft injury and prognosis.
Keywords: histopathology; kidney transplantation; proteinuria; survival.
Copyright © 2016 by the American Society of Nephrology.
Figures
References
-
- Lamb KE, Lodhi S, Meier-Kriesche HU: Long-term renal allograft survival in the United States: a critical reappraisal. Am J Transplant 11: 450–462, 2011 - PubMed
-
- El-Zoghby ZM, Stegall MD, Lager DJ, Kremers WK, Amer H, Gloor JM, Cosio FG: Identifying specific causes of kidney allograft loss. Am J Transplant 9: 527–535, 2009 - PubMed
-
- Sellarés J, de Freitas DG, Mengel M, Reeve J, Einecke G, Sis B, Hidalgo LG, Famulski K, Matas A, Halloran PF: Understanding the causes of kidney transplant failure: the dominant role of antibody-mediated rejection and nonadherence. Am J Transplant 12: 388–399, 2012 - PubMed
-
- Naesens M, Kuypers DR, De Vusser K, Evenepoel P, Claes K, Bammens B, Meijers B, Sprangers B, Pirenne J, Monbaliu D, Jochmans I, Lerut E: The histology of kidney transplant failure: a long-term follow-up study. Transplantation 98: 427–435, 2014 - PubMed
-
- Cravedi P, Ruggenenti P, Remuzzi G: Proteinuria should be used as a surrogate in CKD. Nat Rev Nephrol 8: 301–306, 2012 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
