

Unplanned 30-Day Readmissions in a General Internal Medicine Hospitalist Service at a Comprehensive Cancer Center
- PMID: 26152375
- PMCID: PMC4575406
- DOI: 10.1200/JOP.2014.003087
Unplanned 30-Day Readmissions in a General Internal Medicine Hospitalist Service at a Comprehensive Cancer Center
Abstract
Purpose: Hospital readmissions are considered by the Centers for Medicare and Medicaid as a metric for quality of health care delivery. Robust data on the readmission profile of patients with cancer are currently insufficient to determine whether this measure is applicable to cancer hospitals as well. To address this knowledge gap, we estimated the unplanned readmission rate and identified factors influencing unplanned readmissions in a hospitalist service at a comprehensive cancer center.
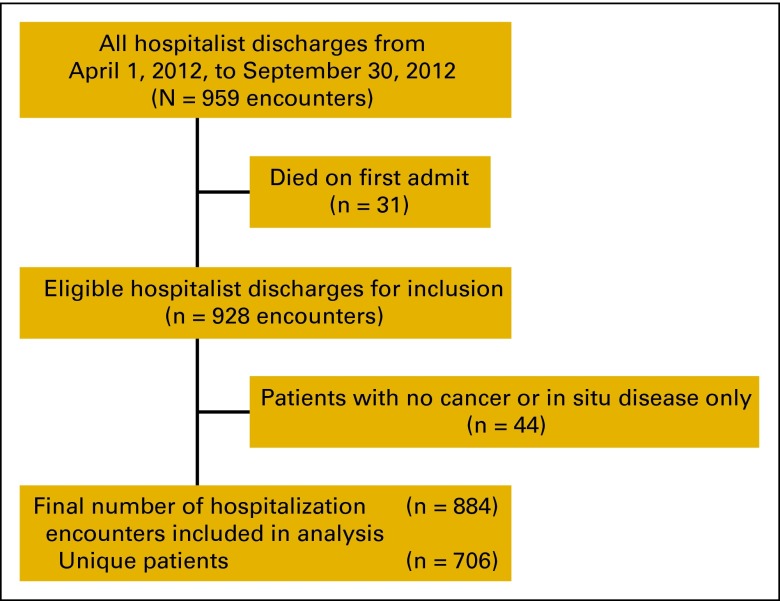
Methods: We retrospectively analyzed unplanned 30-day readmission of patients discharged from the General Internal Medicine Hospitalist Service at a comprehensive cancer center between April 1, 2012, and September 30, 2012. Multiple independent variables were studied using univariable and multivariable logistic regression models, with generalized estimating equations to identify risk factors associated with readmissions.
Results: We observed a readmission rate of 22.6% in our cohort. The median time to unplanned readmission was 10 days. Unplanned readmission was more likely in patients with metastatic cancer and those with three or more comorbidities. Patients discharged to hospice were less likely to be readmitted (all P values < .01).
Conclusion: We observed a high unplanned readmission rate among our population of patients with cancer. The risk factors identified appear to be related to severity of illness and open up opportunities for improving coordination with primary care physicians, oncologists, and other specialists to manage comorbidities, or perhaps transition appropriate patients to palliative care. Our findings will be instrumental for developing targeted interventions to help reduce readmissions at our hospital. Our data also provide direction for appropriate application of readmission quality measures in cancer hospitals.
Copyright © 2015 by American Society of Clinical Oncology.
References
-
- Medicare Payment Advisory Commission. Report to the Congress: Promoting Greater Efficiency in Medicare. Washington, DC: Medicare Payment Advisory Commission; 2007. pp. 103–120.
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–1428. - PubMed
-
- Medicare Payment Advisory Commission. Report to the Congress: Medicare and the Health Care Delivery System. Washington, DC: Medicare Payment Advisory Commission; 2013. pp. 91–114.
-
- Kocher RP, Adashi EY. Hospital readmissions and the Affordable Care Act: Paying for coordinated quality care. JAMA. 2011;306:1794–1795. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
