

Associations of Soluble CD14 and Endotoxin with Mortality, Cardiovascular Disease, and Progression of Kidney Disease among Patients with CKD
- PMID: 26153127
- PMCID: PMC4559509
- DOI: 10.2215/CJN.03100315
Associations of Soluble CD14 and Endotoxin with Mortality, Cardiovascular Disease, and Progression of Kidney Disease among Patients with CKD
Abstract
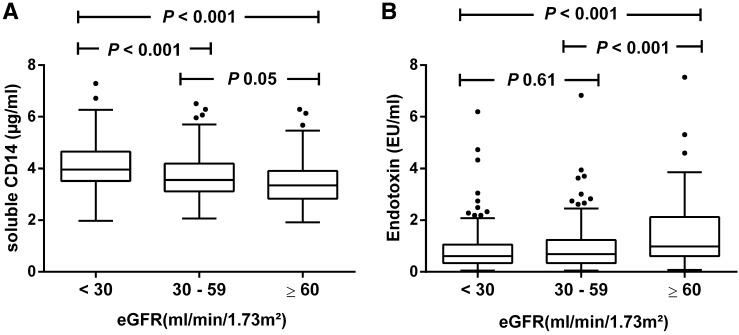
Background and objectives: CD14 plays a key role in the innate immunity as pattern-recognition receptor of endotoxin. Higher levels of soluble CD14 (sCD14) are associated with overall mortality in hemodialysis patients. The influence of kidney function on plasma sCD14 levels and its relationship with adverse outcomes in patients with CKD not yet on dialysis is unknown. This study examines the associations between plasma levels of sCD14 and endotoxin with adverse outcomes in patients with CKD.
Design, setting, participants, & measurements: We measured plasma levels of sCD14 and endotoxin in 495 Leuven Mild-to-Moderate CKD Study participants. Mild-to-moderate CKD was defined as presence of kidney damage or eGFR<60 ml/min per 1.73 m(2) for ≥3 months, with exclusion of patients on RRT. Study participants were enrolled between November 2005 and September 2006.
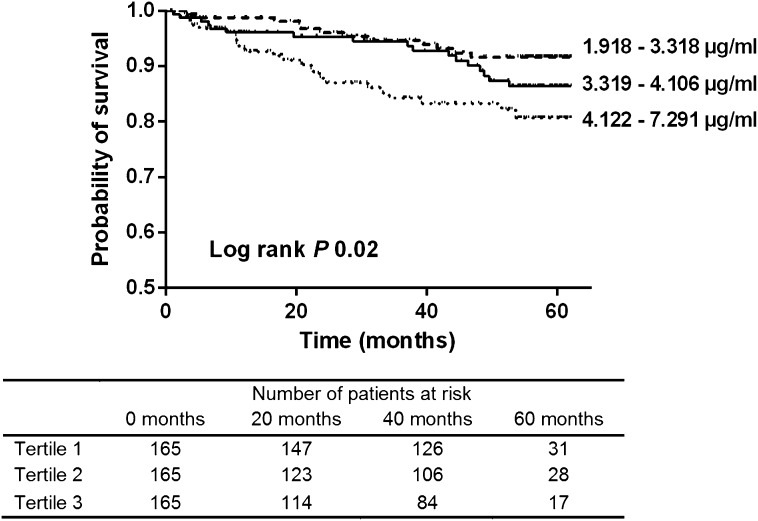
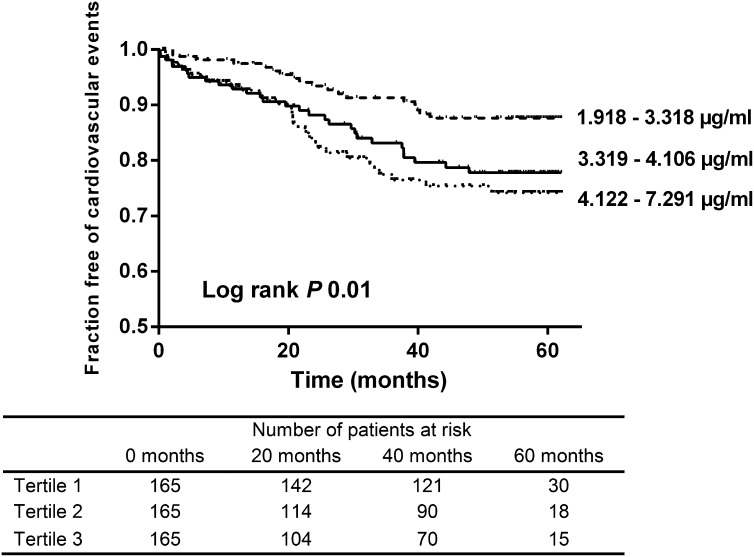
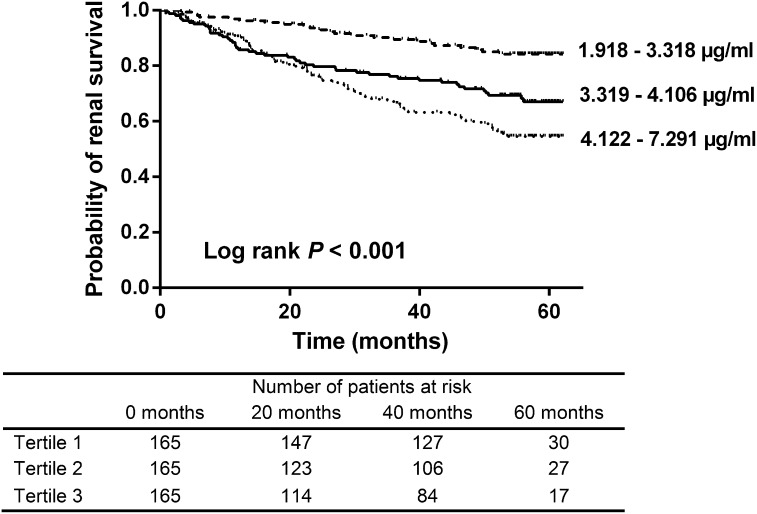
Results: Plasma sCD14 was negatively associated with eGFR (ρ=-0.34, P<0.001). During a median follow-up of 54 (interquartile range, 23-58) months, 53 patients died. Plasma sCD14 was predictive of mortality, even after adjustment for renal function, Framingham risk factors, markers of mineral bone metabolism, and nutritional and inflammatory parameters (hazard ratio [HR] per SD higher of 1.90; 95% confidence interval [95% CI],1.32 to 2.74; P<0.001). After adjustment for the same risk factors, plasma sCD14 was also a predictor of cardiovascular disease (HR, 1.30; 95% CI, 1.00 to 1.69; P=0.05). Although plasma sCD14 was associated with progression of CKD, defined as reaching ESRD or doubling of serum creatinine in models adjusted for CKD-specific risk factors (HR, 1.24; 95% CI, 1.01 to 1.52; P=0.04), significance was lost when adjusted for proteinuria (HR, 1.19; 95% CI, 0.96 to 1.48; P=0.11). There was neither correlation between plasma endotoxin and sCD14 (ρ=-0.06, P=0.20) nor was endotoxin independently associated with adverse outcome during follow-up.
Conclusions: Plasma sCD14 is elevated in patients with decreased kidney function and associated with mortality and cardiovascular disease in patients with CKD not yet on dialysis.
Keywords: CKD; endotoxin; inflammation; microbiome; soluble CD14.
Copyright © 2015 by the American Society of Nephrology.
Figures
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
-
- Berg RD: The indigenous gastrointestinal microflora. Trends Microbiol 4: 430–435, 1996 - PubMed
-
- Vaziri ND, Wong J, Pahl M, Piceno YM, Yuan J, Desantis TZ, Ni Z, Nguyen TH, Andersen GL: Chronic kidney disease alters intestinal microbial flora. Kidney Int 83: 308–315, 2013 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
