

Reducing Medicaid Churning: Extending Eligibility For Twelve Months Or To End Of Calendar Year Is Most Effective
- PMID: 26153313
- PMCID: PMC4664196
- DOI: 10.1377/hlthaff.2014.1204
Reducing Medicaid Churning: Extending Eligibility For Twelve Months Or To End Of Calendar Year Is Most Effective
Abstract
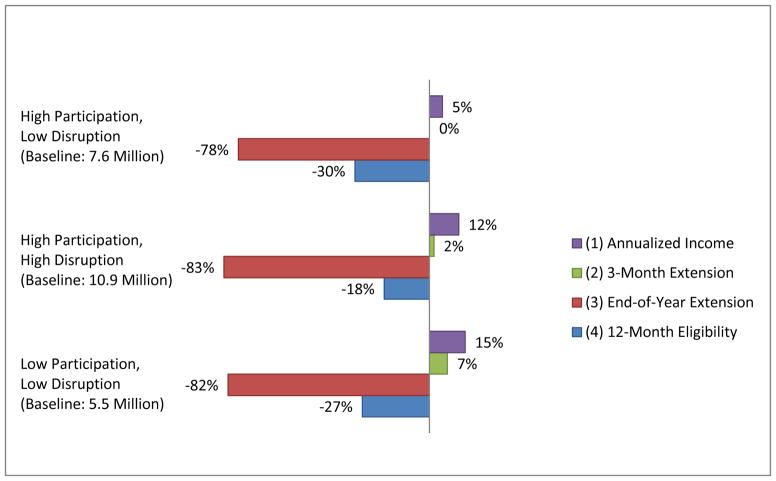
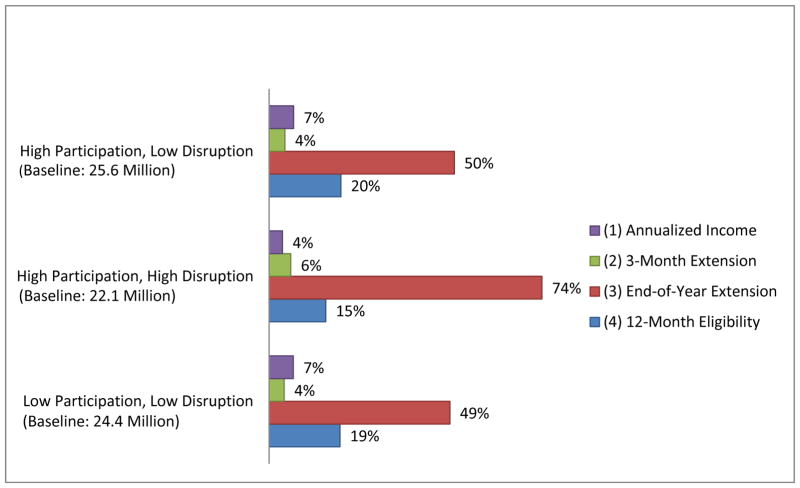
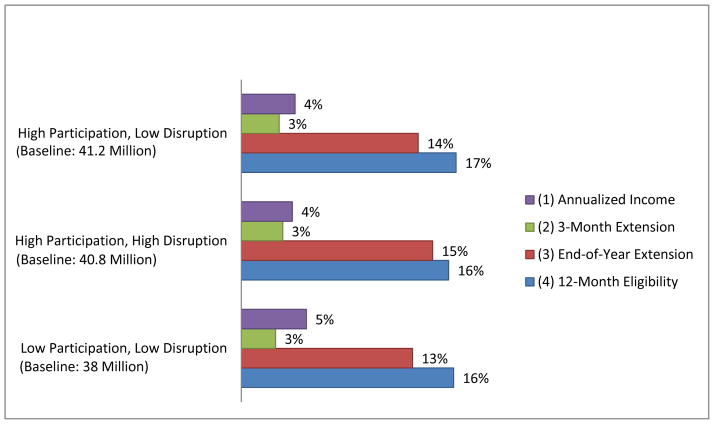
Medicaid churning--the constant exit and reentry of beneficiaries as their eligibility changes--has long been a problem for both Medicaid administrators and recipients. Churning will continue under the Affordable Care Act because, despite new federal rules, Medicaid eligibility will continue to be based on current monthly income. We developed a longitudinal simulation model to evaluate four policy options for modifying or extending Medicaid eligibility to reduce churning. The simulations suggest that two options--extending eligibility either to the end of a calendar year or for twelve months after enrollment--would be the most effective methods for reducing churning. The other options--a three-month extension or eligibility based on projected annual income--would reduce churning to a lesser extent. States should consider implementation of the option that best balances costs while improving access to coverage and, thereby, the health of Medicaid enrollees.
Keywords: Health Reform; Medicaid.
Project HOPE—The People-to-People Health Foundation, Inc.
Figures
Similar articles
-
Medicaid and marketplace eligibility changes will occur often in all states; policy options can ease impact.Health Aff (Millwood). 2014 Apr;33(4):700-7. doi: 10.1377/hlthaff.2013.1023. Epub 2014 Mar 12. Health Aff (Millwood). 2014. PMID: 24622387
-
Insurance Churning Rates For Low-Income Adults Under Health Reform: Lower Than Expected But Still Harmful For Many.Health Aff (Millwood). 2016 Oct 1;35(10):1816-1824. doi: 10.1377/hlthaff.2016.0455. Health Aff (Millwood). 2016. PMID: 27702954
-
Crossing 138: two approaches to churn under the Affordable Care Act.Health Matrix Clevel. 2014;24:109-41. Health Matrix Clevel. 2014. PMID: 25112137
-
Health care coverage for children who are on and off welfare.Future Child. 1997 Spring;7(1):87-98. Future Child. 1997. PMID: 9170735 Review.
-
Current Evidence to Guide Practice, Policy, and Research: Extending Medicaid Coverage in the Postpartum Period.J Obstet Gynecol Neonatal Nurs. 2023 Jan;52(1):95-101. doi: 10.1016/j.jogn.2022.11.006. Epub 2022 Dec 2. J Obstet Gynecol Neonatal Nurs. 2023. PMID: 36463951 Review.
Cited by
-
Impact of a statewide Emergency Department Information Exchange on health care use and expenditures.Health Serv Res. 2022 Jun;57(3):603-613. doi: 10.1111/1475-6773.13963. Epub 2022 Mar 13. Health Serv Res. 2022. PMID: 35235203 Free PMC article.
-
Preventive Care Use Among Justice-Involved and Non-Justice-Involved Youth.Pediatrics. 2017 Nov;140(5):e20171107. doi: 10.1542/peds.2017-1107. Epub 2017 Oct 2. Pediatrics. 2017. PMID: 28970371 Free PMC article.
-
Primary care visits and ambulatory care sensitive diabetes hospitalizations among adult Alabama Medicaid beneficiaries.Prim Care Diabetes. 2022 Feb;16(1):116-121. doi: 10.1016/j.pcd.2021.10.005. Epub 2021 Nov 9. Prim Care Diabetes. 2022. PMID: 34772648 Free PMC article.
-
Ensuring access to high-quality substance use disorder treatment for Medicaid enrollees: A qualitative study of diverse stakeholders' perspectives.J Subst Abuse Treat. 2021 Oct;129:108511. doi: 10.1016/j.jsat.2021.108511. Epub 2021 May 31. J Subst Abuse Treat. 2021. PMID: 34176694 Free PMC article.
-
State Approaches to Simplify Medicaid Eligibility and Implications for Inequality of Infant Health.RSF. 2023 Sep;9(4):32-60. doi: 10.7758/rsf.2023.9.4.02. RSF. 2023. PMID: 39703714 Free PMC article.
References
Endnotes
-
- Sommers BD. Why millions of children eligible for Medicaid and SCHIP are uninsured: poor retention versus poor take-Up. Health Aff (Millwood) 2007;26(5):w560–7. - PubMed
-
- Fairbrother G, Dutton MJ, Bachrach D, Newall KA, Boozang P, Cooper R. Costs of enrolling children in Medicaid and SCHIP. Health Aff (Millwood) 2004;23(1):237–243. - PubMed
-
- Hill I, Lutzky AW. Understanding SCHIP Retention. Washington (DC): Urban Institute; 2003. Is there a hole in the bucket?
-
- Perry M, Kannel S, Riley T, Pernice C. What parents say: why eligible children lose SCHIP. Portland (ME): National Academy for State Health Policy; 2001.
References for Appendix
-
- Kaiser Commission on Medicaid and the Uninsured. Holding Steady, Looking Ahead: Annual Findings of a 50-State Survey of Eligibility Rules, Enrollment and Renewal Procedures, and Cost-Sharing Practices in Medicaid and CHIP, 2010–2011. 2011 Publication #8130, Jan. Available at: http://kaiserfamilyfoundation.files.wordpress.com/2013/01/8130.pdf.
-
- Sommers BD, Swartz K, Epstein AM. Policy Makers Should Prepare for Major Uncertainties in Medicaid Enrollment, Costs, and Needs for Physicians Under Health Reform. Health Affairs. 2011;30(11):2186–93. - PubMed
-
- Elmendorf DW. Testimony Statement of Douglas W. Elmendorf, Director. Congressional Budget Office, before the Subcommittee on Health, Committee on Energy and Commerce, U.S. House of Representatives, “CBO’s Analysis of the Major Health Care Legislation Enacted in March 2010. 2011 Mar 30; Available at: http://www.cbo.gov/sites/default/files/03-30-healthcarelegislation.pdf.
-
- Kaiser Family Foundation. Medicaid Coverage and Spending in Health Reform: National and State by State Results for Adults At or Below 133% FPL. 2010 May; Available at: http://www.kff.org/healthreform/upload/Medicaid-Coverage-and-Spending-in....
-
- Sommers BD, Epstein AM. Medicaid Expansion – the Soft Underbelly of Health Care Reform? New England Journal of Medicine. 2010;363(22):2085–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical