

The indolent nature of pulmonary metastases from ductal adenocarcinoma of the pancreas
- PMID: 26153355
- PMCID: PMC4509861
- DOI: 10.1002/jso.23943
The indolent nature of pulmonary metastases from ductal adenocarcinoma of the pancreas
Abstract
Background and objectives: The natural history of pulmonary metastases from pancreatic ductal adenocarcinoma (PDAC) is not well studied. Limited evidence suggests patients with isolated pulmonary metastases from PDAC follow a more benign clinical course than those with other sites of metastases.
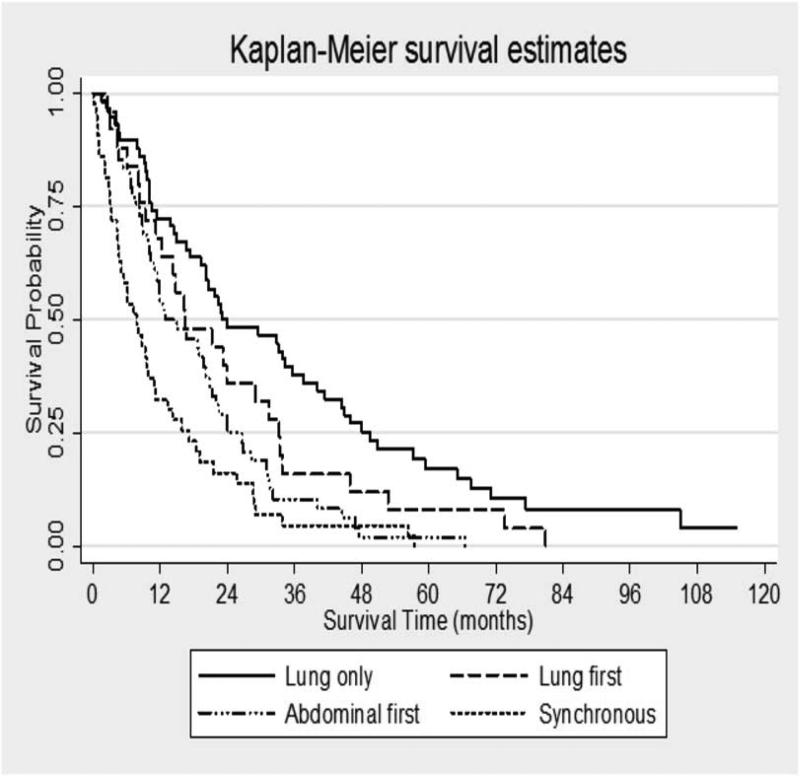
Methods: We performed a retrospective review of all patients with pulmonary metastases from PDAC from 2000 to 2010 and analyzed survival utilizing the Kaplan-Meier method based upon location of first metastasis (lung first, intra-abdominal first, or synchronous intra-abdominal and lung metastases).
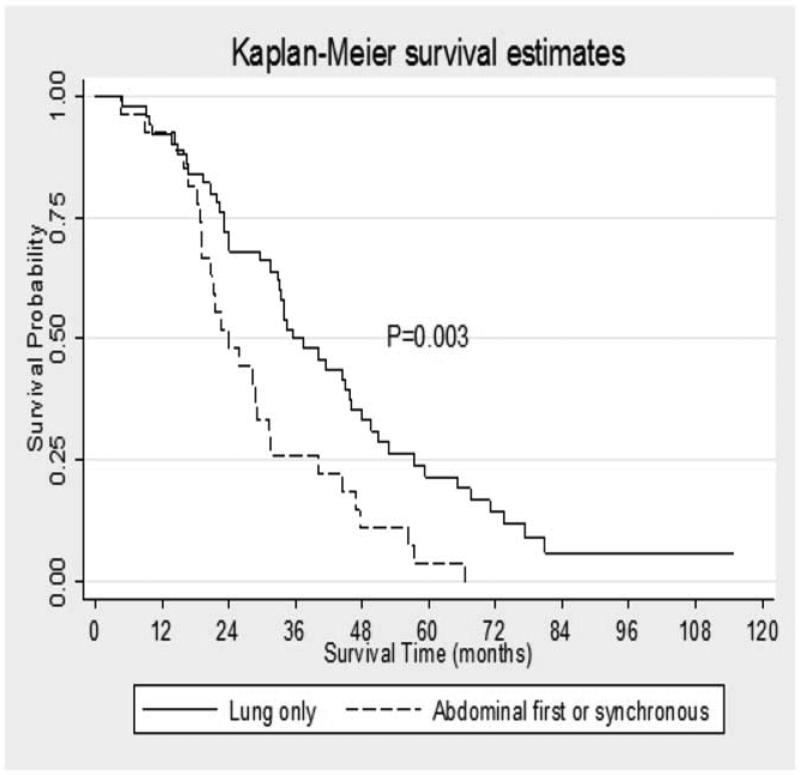
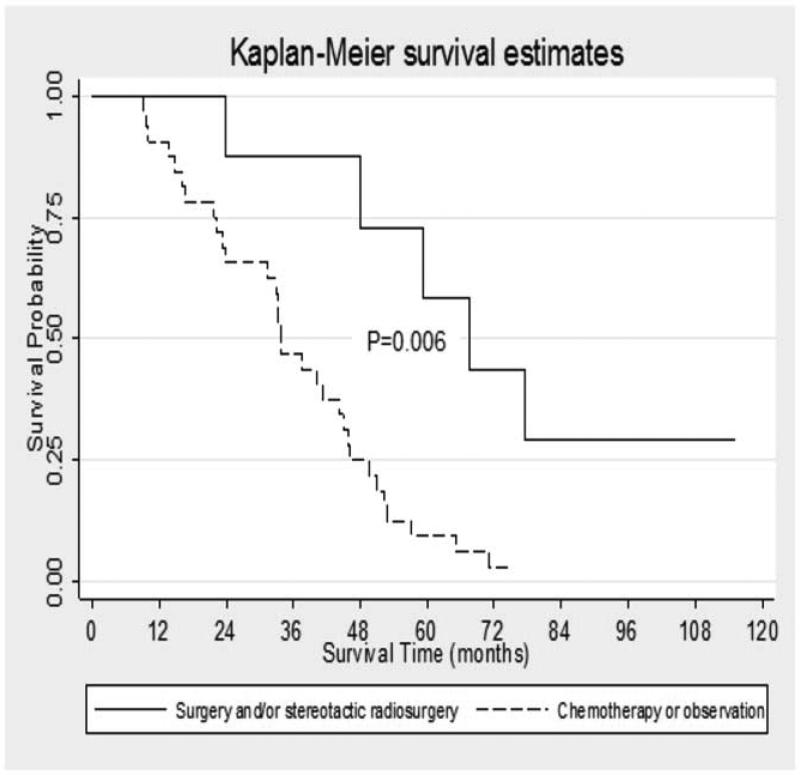
Results: Median survival among subjects with lung as the only site of metastases was significantly longer than those with other metastatic patterns. In subjects that had undergone resection of their PDAC, survival in those with lung as a first site of recurrence remained significantly longer than those with abdominal first or synchronous intra-abdominal and lung recurrence. Among resected patients that developed lung only recurrence, survival was significantly prolonged (67.5 months) in those who underwent surgical resection/stereotactic radiosurgery compared to chemotherapy (33.8 months) or observation (29.9 months) for treatment of lung recurrence.
Conclusion: Patients with isolated pulmonary recurrence from PDAC may realize a survival benefit from surgical intervention or stereotactic radiosurgery compared to chemotherapy or observation for treatment of lung recurrence.
Keywords: lung metastases; pancreatic ductal adenocarcinoma; pulmonary metastases.
© 2015 Wiley Periodicals, Inc.
Figures
References
-
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA: a cancer journal for clinicians. 2014;64:9–29. - PubMed
-
- Bilimoria KY, Bentrem DJ, Ko CY, Ritchey J, Stewart AK, Winchester DP, et al. Validation of the 6th edition AJCC Pancreatic Cancer Staging System: report from the National Cancer Database. Cancer. 2007;110:738–744. - PubMed
-
- Samuel N, Hudson TJ. The molecular and cellular heterogeneity of pancreatic ductal adenocarcinoma. Nature reviews Gastroenterology & hepatology. 2012;9:77–87. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
