

Explaining the Decrease of In-Hospital Mortality from Ischemic Stroke
- PMID: 26154704
- PMCID: PMC4496086
- DOI: 10.1371/journal.pone.0131473
Explaining the Decrease of In-Hospital Mortality from Ischemic Stroke
Abstract
Background: Mortality from ischemic stroke has declined over time. However, little is known about the reasons for the decreased mortality. We therefore aimed to evaluate trends in in-hospital mortality and to identify factors associated with these trends.
Methods: This study was based on a prospective database of 26 hospitals of the Stroke Register of Northwestern Germany, which included 73,614 patients admitted between 2000 and 2011. Time trends in observed (crude) and risk-adjusted in-hospital mortality were assessed. Independent factors associated with death after stroke were evaluated using multivariable logistic regression analysis.
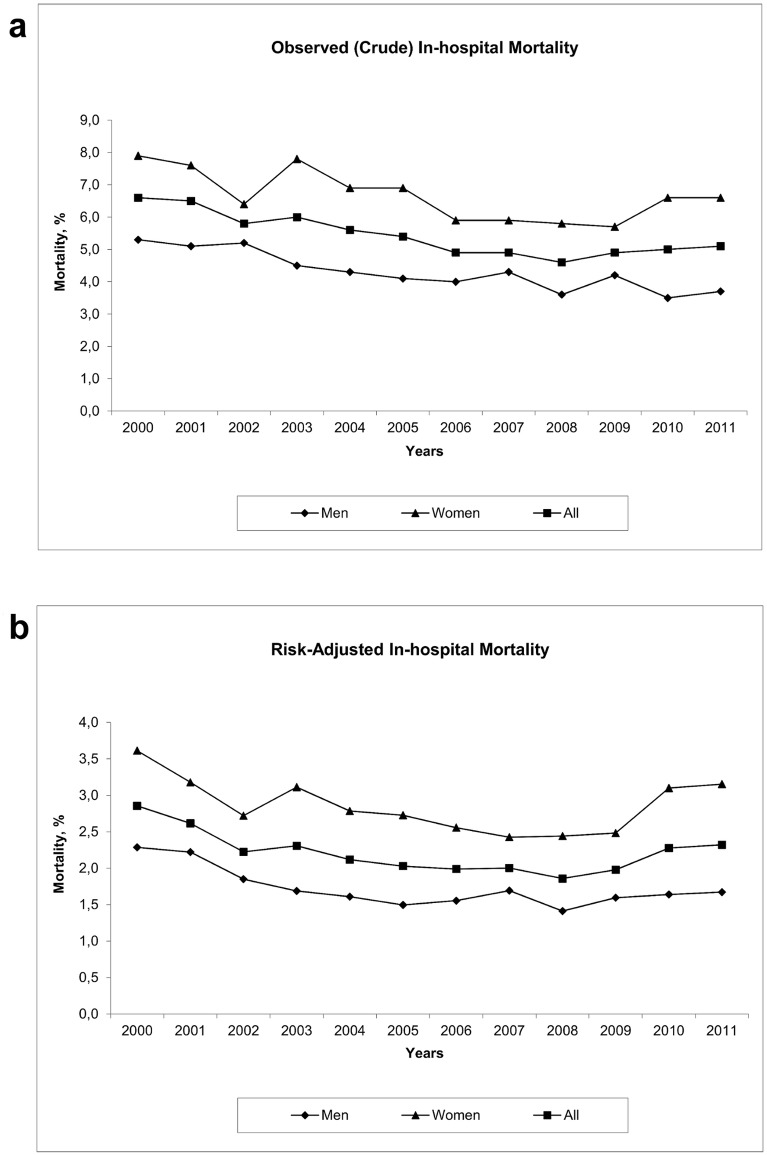
Results: The observed in-hospital mortality decreased from 6.6% in 2000 to 4.6% in 2008 (P < 0.001 for trend) and then remained fairly stable. The risk-adjusted mortality decreased from 2.85% in 2000 to 1.86% in 2008 (P < 0.01 for trend) and then increased to 2.32% in 2011. Use of in-hospital treatments including antiplatelets within 48 hours, antihypertensive therapy, statins, antidiabetics, physiotherapy and anticoagulants increased over time and was significantly associated with a decrease in mortality. The association of the year of admission with mortality became insignificant after adjustment for antiplatelet therapy within 48 hours (from OR 0.96; 95% CI, 0.94-0.98, to OR 0.99; 95% CI, 0.97-1.01) and physiotherapy (from OR 0.96; 95% CI, 0.94-0.97, to OR 0.99; 95% CI, 0.97-1.00).
Conclusions: In-hospital mortality decreased by approximately one third between 2000 and 2008. This decline was paralleled by improvements in different in-hospital managements, and we demonstrated that it was partly mediated by early antiplatelet therapy and physiotherapy use.
Conflict of interest statement
Figures
Similar articles
-
Predictors of in-hospital mortality and attributable risks of death after ischemic stroke: the German Stroke Registers Study Group.Arch Intern Med. 2004 Sep 13;164(16):1761-8. doi: 10.1001/archinte.164.16.1761. Arch Intern Med. 2004. PMID: 15364669
-
Thrombocytopenia and in-hospital mortality risk among ischemic stroke patients.J Stroke Cerebrovasc Dis. 2013 Oct;22(7):e99-e102. doi: 10.1016/j.jstrokecerebrovasdis.2012.08.005. Epub 2012 Sep 10. J Stroke Cerebrovasc Dis. 2013. PMID: 22974703
-
Time trends in systemic thrombolysis in a large hospital-based stroke registry.Cerebrovasc Dis. 2012;33(4):316-21. doi: 10.1159/000335816. Epub 2012 Feb 15. Cerebrovasc Dis. 2012. PMID: 22343969
-
Stroke unit care and trends of in-hospital mortality for stroke in Germany 2005-2010.Int J Stroke. 2014 Apr;9(3):260-5. doi: 10.1111/ijs.12193. Epub 2013 Nov 10. Int J Stroke. 2014. PMID: 24206775
-
Ischemic stroke history predicts increased cardiovascular mortality in chronic heart failure.Anadolu Kardiyol Derg. 2011 Aug;11(5):421-7. doi: 10.5152/akd.2011.109. Epub 2011 Jun 28. Anadolu Kardiyol Derg. 2011. PMID: 21712170
Cited by
-
Temporal profiles of blood pressure, circulating nitric oxide, and adrenomedullin as predictors of clinical outcome in acute ischemic stroke patients.Mol Med Rep. 2016 May;13(5):3724-34. doi: 10.3892/mmr.2016.5001. Epub 2016 Mar 18. Mol Med Rep. 2016. PMID: 27035412 Free PMC article. Clinical Trial.
-
Relationship Between the Hemoglobin-to-Red Cell Distribution Width Ratio and All-Cause Mortality in Ischemic Stroke Patients with Atrial Fibrillation: An Analysis from the MIMIC-IV Database.Neuropsychiatr Dis Treat. 2022 Feb 18;18:341-354. doi: 10.2147/NDT.S350588. eCollection 2022. Neuropsychiatr Dis Treat. 2022. PMID: 35221686 Free PMC article.
-
C-reactive protein for predicting all-cause mortality in patients with acute ischemic stroke: a meta-analysis.Biosci Rep. 2019 Feb 19;39(2):BSR20181135. doi: 10.1042/BSR20181135. Print 2019 Feb 28. Biosci Rep. 2019. PMID: 30718369 Free PMC article.
-
End-of-life decisions in acute stroke patients: an observational cohort study.BMC Palliat Care. 2016 Apr 5;15:38. doi: 10.1186/s12904-016-0113-8. BMC Palliat Care. 2016. PMID: 27044257 Free PMC article.
-
Stroke History is an Independent Risk Factor for Poor Prognosis in Ischemic Stroke Patients: Results from a Large Nationwide Stroke Registry.Curr Neurovasc Res. 2020;17(4):487-494. doi: 10.2174/1567202617666200817141837. Curr Neurovasc Res. 2020. PMID: 32807054 Free PMC article.
References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. (2012) Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380: 2095–2128. 10.1016/S0140-6736(12)61728-0 - DOI - PMC - PubMed
-
- Carandang R, Seshadri S, Beiser A, Kelly-Hayes M, Kase CS, Kannel WB, et al. (2006) Trends in incidence, lifetime risk, severity, and 30-day mortality of stroke over the past 50 years. JAMA 296: 2939–2946.. - PubMed
-
- Jauch EC, Saver JL, Adams HP Jr, Bruno A, Connors JJB, Demaerschalk BM, et al. (2013) Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the american heart association/american stroke association. Stroke 44: 870–947. 10.1161/STR.0b013e318284056a - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
