

Atrial Fibrillation Is an Independent Predictor of Mortality in Critically Ill Patients
- PMID: 26154932
- PMCID: PMC4725582
- DOI: 10.1097/CCM.0000000000001166
Atrial Fibrillation Is an Independent Predictor of Mortality in Critically Ill Patients
Abstract
Objectives: Atrial fibrillation has been associated with increased mortality in critically ill patients. We sought to determine whether atrial fibrillation in the ICU is an independent risk factor for death. A secondary objective was to determine if patients with new-onset atrial fibrillation have different risk factors or outcomes compared with patients with a previous history of atrial fibrillation.
Design: Prospective observational cohort study.
Setting: Medical and general surgical ICUs in a tertiary academic medical center.
Patients: One thousand seven hundred seventy critically ill patients requiring at least 2 days in the ICU.
Interventions: None.
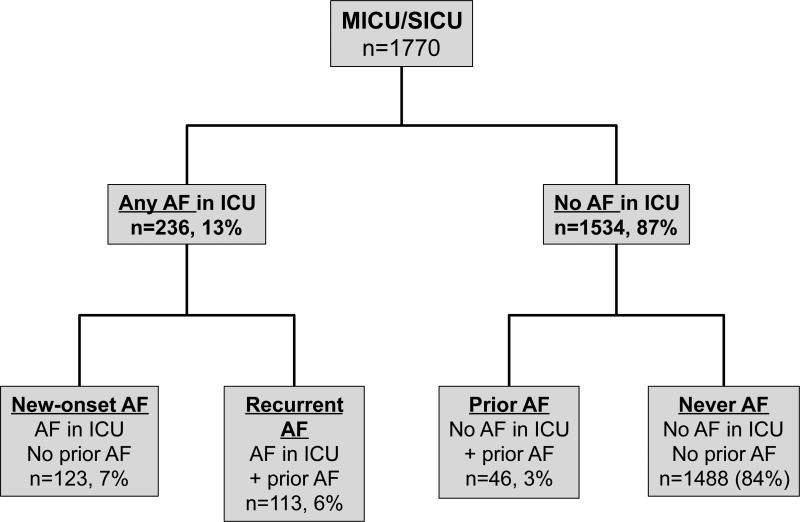
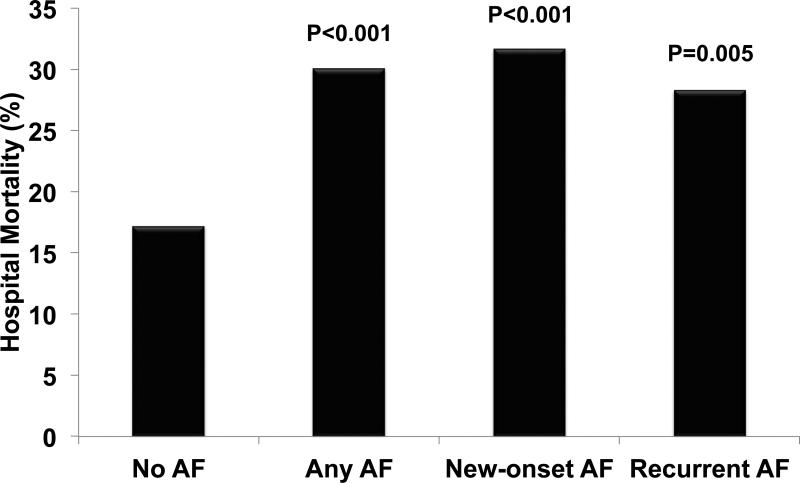
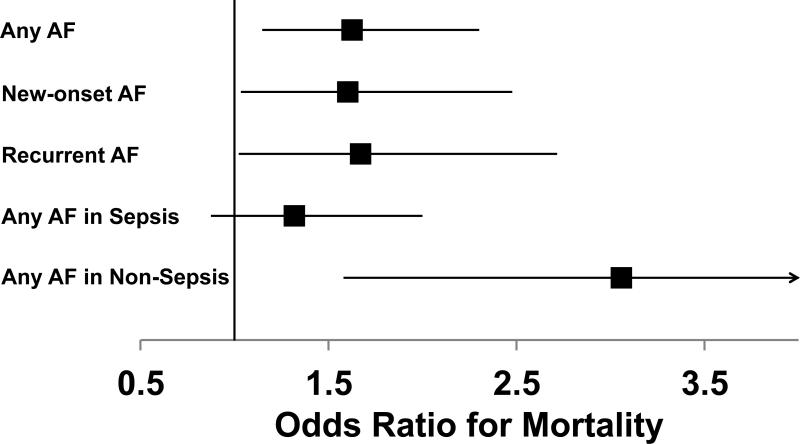
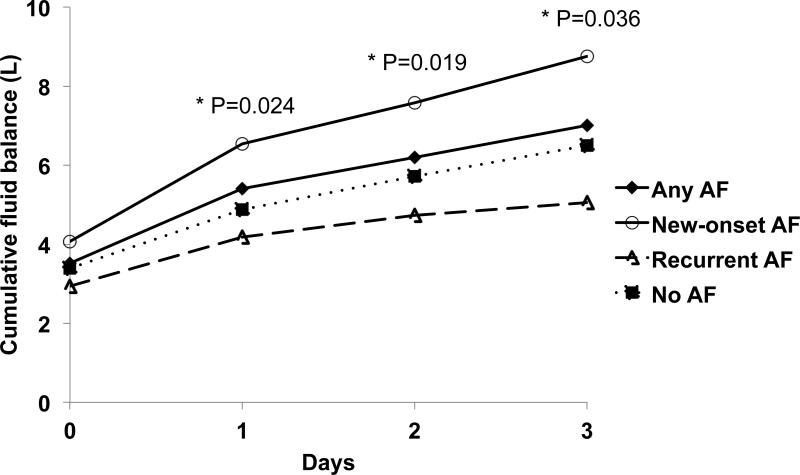
Measurements and main results: Demographics, medical history, development of atrial fibrillation, fluid balance, echocardiographic findings, medication administration, and hospital mortality were collected during the first 4 days of ICU admission. Atrial fibrillation occurred in 236 patients (13%) (Any AF). Of these, 123 patients (7%) had no prior atrial fibrillation (New-onset AF) while the remaining 113 (6%) had recurrent atrial fibrillation (Recurrent AF). Any AF was associated with male gender, Caucasian race, increased age, cardiac disease, organ failures, and disease severity. Patients with Any AF had increased mortality compared with those without atrial fibrillation (31% vs 17%; p < 0.001), and Any AF was independently associated with death (odds ratio, 1.62; 95% CI, 1.14-2.29; p = 0.007) in multivariable analysis controlling for severity of illness and other confounders. The association of atrial fibrillation with death was magnified in patients without sepsis (odds ratio, 2.92; 95% CI, 1.52-5.60; p = 0.001). Treatment for atrial fibrillation had no effect on hospital mortality. New-onset AF and Recurrent AF were each associated with increased mortality. New-onset AF, but not Recurrent AF, was associated with increased diastolic dysfunction and vasopressor use and a greater cumulative positive fluid balance.
Conclusions: Atrial fibrillation in critical illness, whether new-onset or recurrent, is independently associated with increased hospital mortality, especially in patients without sepsis.
Figures
Comment in
-
Atrial Fibrillation in Critical Illness: Innocent Bystander or Guilty Party?Crit Care Med. 2015 Oct;43(10):2254-5. doi: 10.1097/CCM.0000000000001207. Crit Care Med. 2015. PMID: 26376252 No abstract available.
-
New-Onset Atrial Fibrillation in Sepsis: So Common, but So Different.Crit Care Med. 2016 May;44(5):e306-7. doi: 10.1097/CCM.0000000000001541. Crit Care Med. 2016. PMID: 27083028 No abstract available.
-
The authors reply.Crit Care Med. 2016 May;44(5):e307. doi: 10.1097/CCM.0000000000001579. Crit Care Med. 2016. PMID: 27083029 No abstract available.
References
-
- Annane D, Sebille V, Duboc D, Le Heuzey JY, Sadoul N, Bouvier E, Bellissant E. Incidence and prognosis of sustained arrhythmias in critically ill patients. Am J Respir Crit Care Med. 2008;178(1):20–25. - PubMed
-
- Artucio H, Pereira M. Cardiac arrhythmias in critically ill patients: Epidemiologic study. Crit Care Med. 1990;18(12):1383–1388. - PubMed
-
- Brathwaite D, Weissman C. The new onset of atrial arrhythmias following major noncardiothoracic surgery is associated with increased mortality. Chest. 1998;114(2):462–468. - PubMed
-
- Christian SA, Schorr C, Ferchau L, Jarbrink ME, Parrillo JE, Gerber DR. Clinical characteristics and outcomes of septic patients with new-onset atrial fibrillation. J Crit Care. 2008;23(4):532–536. - PubMed
-
- Goodman S, Shirov T, Weissman C. Supraventricular arrhythmias in intensive care unit patients: Short and long-term consequences. Anesth Analg. 2007;104(4):880–886. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
