

Clinical features and survival outcome of locally advanced extrahepatic cholangiocarcinoma
- PMID: 26155239
- PMCID: PMC4492336
- DOI: 10.14701/kjhbps.2014.18.1.1
Clinical features and survival outcome of locally advanced extrahepatic cholangiocarcinoma
Abstract
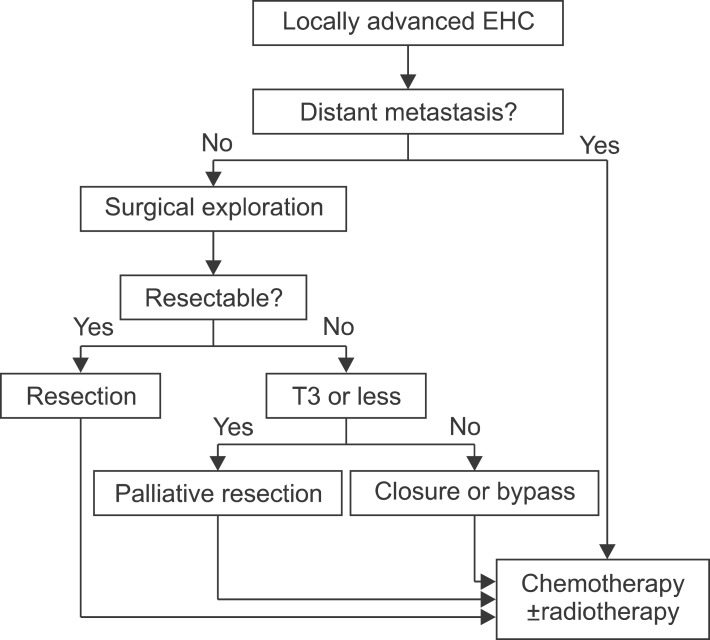
Backgrounds/aims: Little is known about clinical features and survival outcome in locally advanced unresectable extrahepatic cholangiocarcinoma (EHC). The aim was to investigate the clinical features and the survival outcome in these patients, and to evaluate the role of palliative resections in locally advanced unresectable EHC.
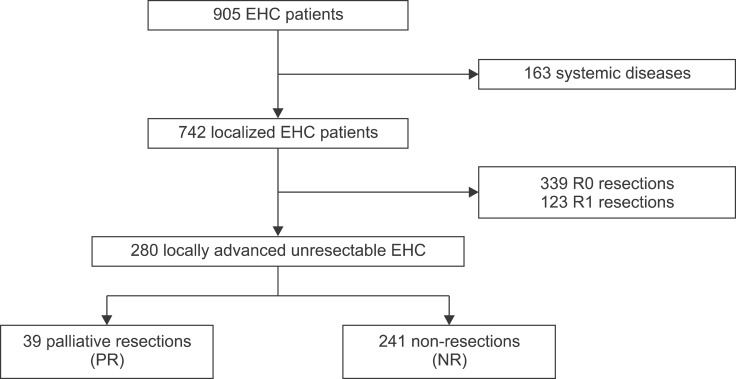
Methods: Between 1995 and 2007, 280 patients with locally advanced unresectable EHC were identified. Clinical, pathologic, and survival data were investigated. A comparative analysis was done between those who received palliative resection (PR) and those who were not operated on (NR).
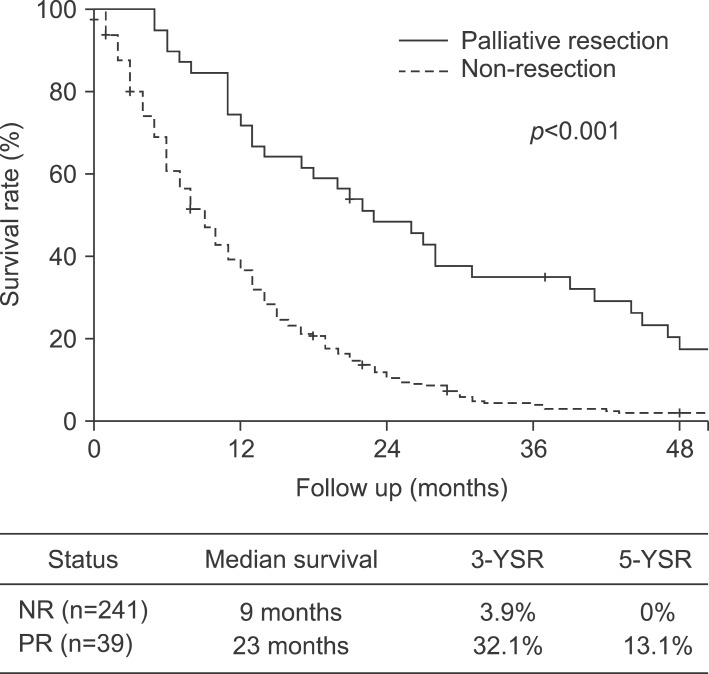
Results: The overall median survival of the study population was 10±1 months, and the 3- and 5-year survival rates (YSR) were 8.5% and 2.5%, respectively. The median survival, 3- and 5-YSR of PR were 23 months, 32.1% and 13.1%, respectively. For NR, they were 9 months, 3.9% and 0%, which were significantly worse than PR (p<0.001). In univariate analysis, T classification, N classification, tumor location, palliative resection, adjuvant treatment, chemotherapy, and radiation therapy were factors that showed survival difference between PR and NR. Regional lymph node metastasis (RR, 2.084; 95% CI, 1.491-2.914; p<0.001), non-resections (RR, 2.270; 95% CI, 1.497-3.443; p<0.001), and no chemotherapy (RR, 1.604; 95% CI, 1.095-2.349; p=0.015) were identified as risk factors for poor outcome on multivariate analysis.
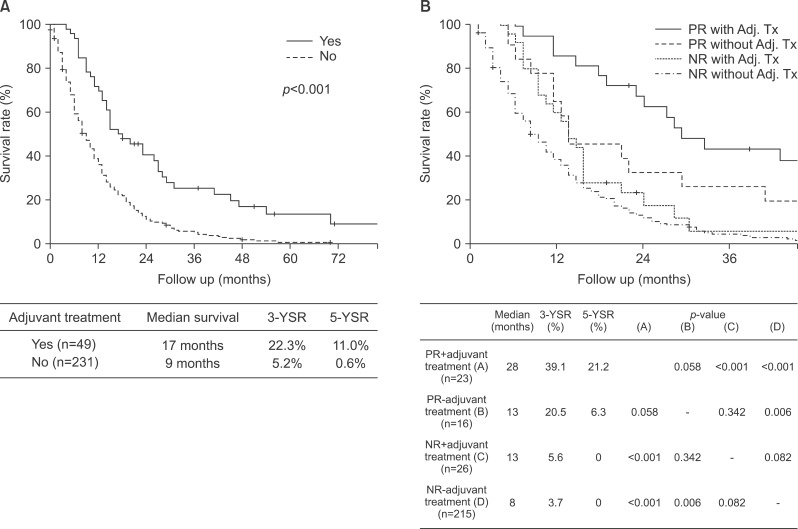
Conclusions: Without evidence of systemic disease, palliative resection may provide some survival benefit in selected locally advanced unresectable EHCs and adjuvant treatment may further improve survival outcome.
Keywords: Adjuvant therapy; Cholangiocarcinoma; Extrahepatic; Palliative surgery; Survival.
Figures
Similar articles
-
Comparison of external beam radiation and brachytherapy to external beam radiation alone for unresectable extrahepatic cholangiocarcinoma.J Gastrointest Oncol. 2016 Aug;7(4):580-7. doi: 10.21037/jgo.2016.03.14. J Gastrointest Oncol. 2016. PMID: 27563448 Free PMC article.
-
Comparison of resection and transarterial chemoembolisation in the treatment of advanced intrahepatic cholangiocarcinoma--a single-center experience.Eur J Surg Oncol. 2013 Jun;39(6):593-600. doi: 10.1016/j.ejso.2013.03.010. Epub 2013 Apr 20. Eur J Surg Oncol. 2013. PMID: 23611755
-
Adjuvant Chemotherapy and Radiation Therapy is Associated with Improved Survival for Patients with Extrahepatic Cholangiocarcinoma.Ann Surg Oncol. 2015 Dec;22 Suppl 3:S1133-9. doi: 10.1245/s10434-015-4599-8. Epub 2015 May 15. Ann Surg Oncol. 2015. PMID: 25976862
-
External radiotherapy and brachytherapy in the management of extrahepatic and intrahepatic cholangiocarcinoma: available evidence.Br J Radiol. 2017 Aug;90(1076):20170061. doi: 10.1259/bjr.20170061. Epub 2017 May 23. Br J Radiol. 2017. PMID: 28466653 Free PMC article. Review.
-
Radioembolization for Unresectable Intrahepatic Cholangiocarcinoma: Review of Safety, Response Evaluation Criteria in Solid Tumors 1.1 Imaging Response and Survival.Cancer Biother Radiopharm. 2017 Jun;32(5):161-168. doi: 10.1089/cbr.2017.2189. Epub 2017 Jun 9. Cancer Biother Radiopharm. 2017. PMID: 28598685 Review.
References
-
- Shaib Y, El-Serag HB. The epidemiology of cholangiocarcinoma. Semin Liver Dis. 2004;24:115–125. - PubMed
-
- Vern-Gross TZ, Shivnani AT, Chen K, et al. Survival outcomes in resected extrahepatic cholangiocarcinoma: effect of adjuvant radiotherapy in a surveillance, epidemiology, and end results analysis. Int J Radiat Oncol Biol Phys. 2011;81:189–198. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials