

Th22 cells increase in poor prognosis multiple myeloma and promote tumor cell growth and survival
- PMID: 26155400
- PMCID: PMC4485827
- DOI: 10.1080/2162402X.2015.1005460
Th22 cells increase in poor prognosis multiple myeloma and promote tumor cell growth and survival
Abstract
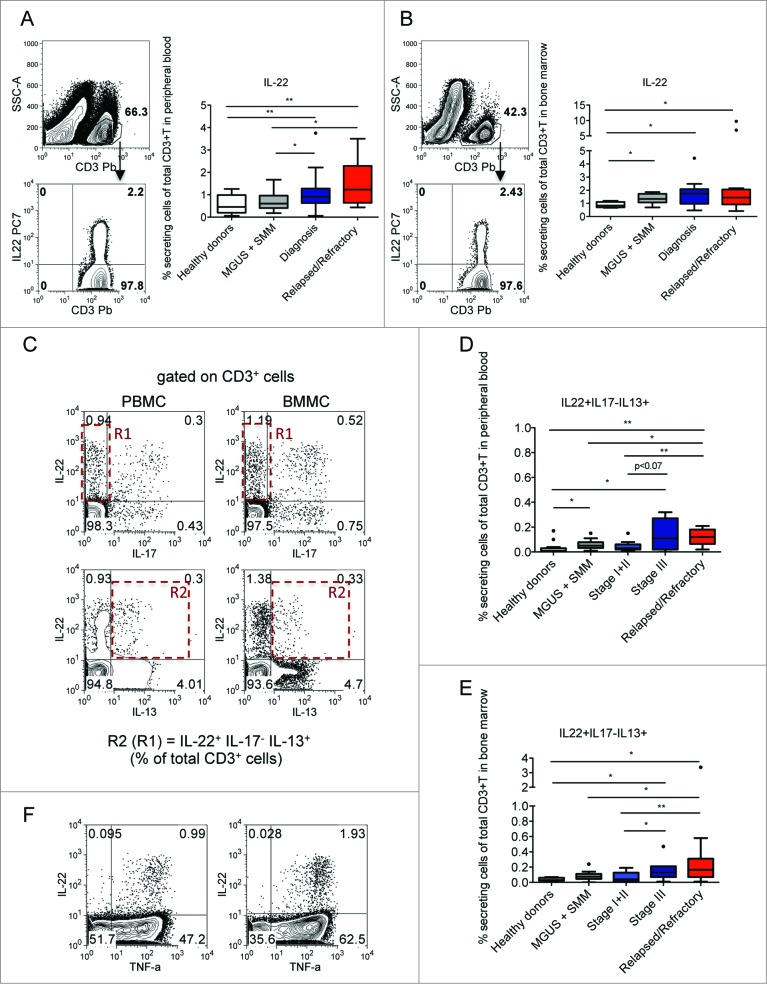
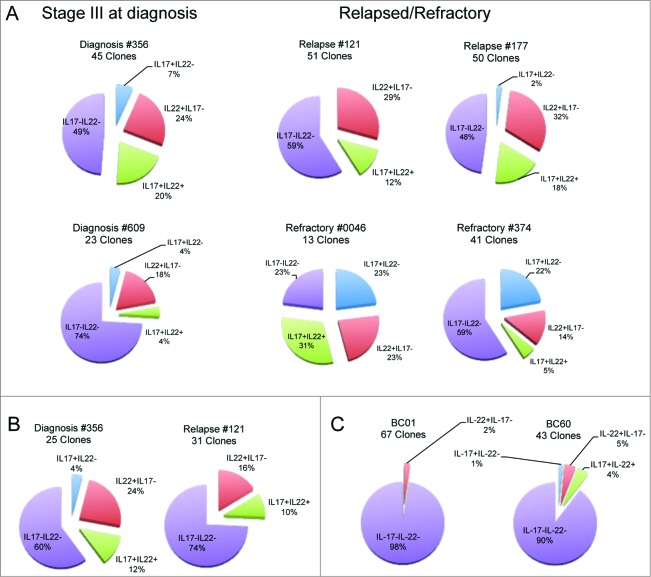
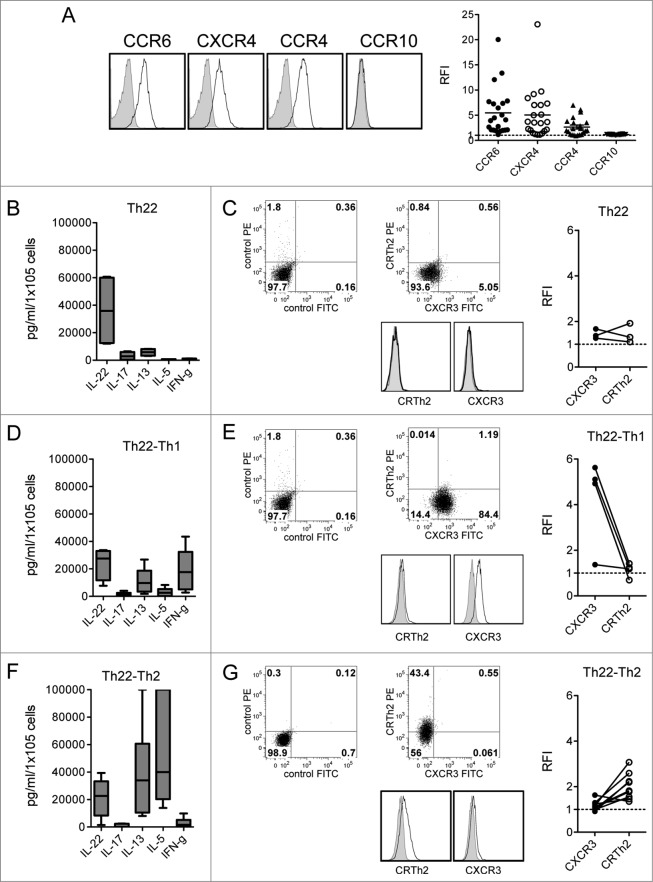
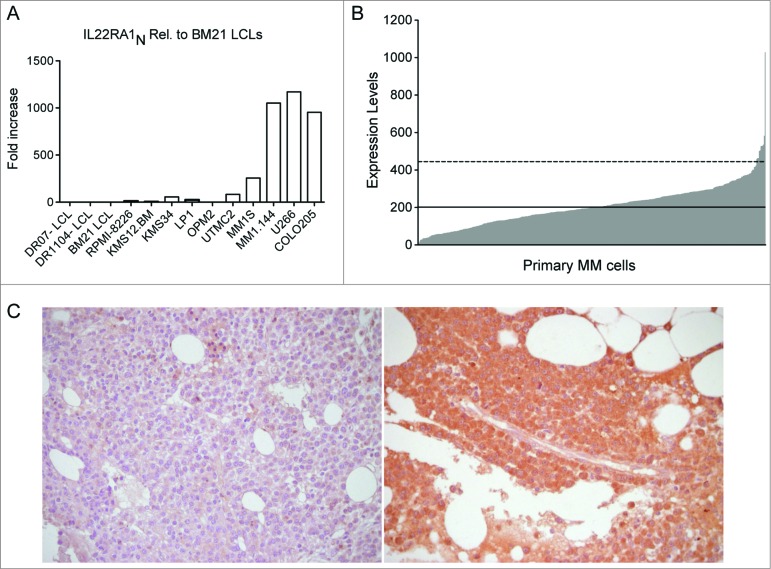
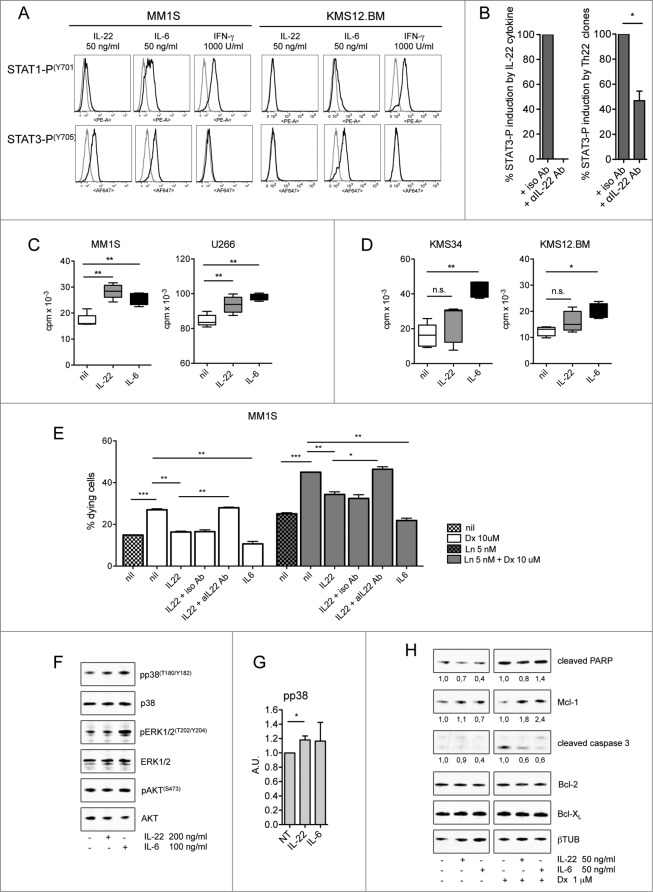
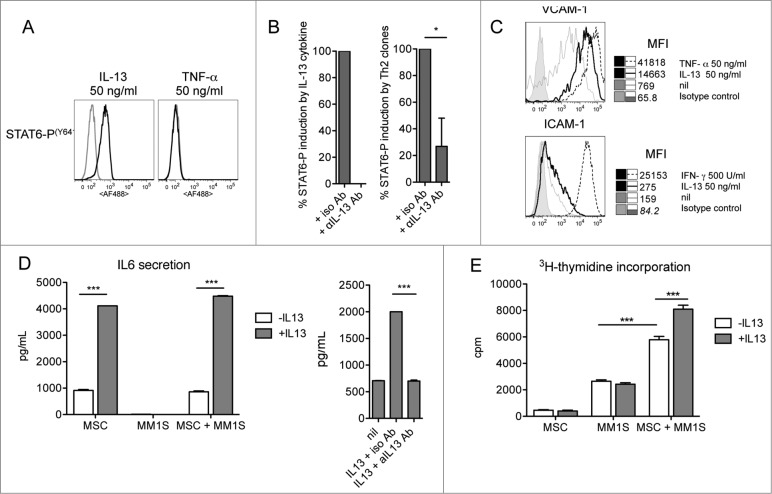
There is increased production of plasmacytoid dendritic cells (pDCs) in the bone marrow (BM) of multiple myeloma (MM) patients and these favor Th22 cell differentiation. Here, we found that the frequency of interleukin (IL)-22+IL-17-IL-13+ T cells is significantly increased in peripheral blood (PB) and BM of stage III and relapsed/refractory MM patients compared with healthy donors and patients with asymptomatic or stage I/II disease. Th22 cells cloned from the BM of MM patients were CCR6+CXCR4+CCR4+CCR10- and produced IL-22 and IL-13 but not IL-17. Furthermore, polyfunctional Th22-Th2 and Th22-Th1 clones were identified based on the co-expression of additional chemokine receptors and cytokines (CRTh2 or CXCR3 and IL-5 or interferon gamma [IFNγ], respectively). A fraction of MM cell lines and primary tumors aberrantly expressed the IL-22RA1 and IL-22 induced STAT-3 phosphorylation, cell growth, and resistance to drug-induced cell death in MM cells. IL-13 treatment of normal BM mesenchymal stromal cells (MSCs) induced STAT-6 phosphorylation, adhesion molecule upregulation, and increased IL-6 production and significantly favored MM cell growth compared with untreated BM MSCs. Collectively, our data show that increased frequency of IL-22+IL-17-IL-13+ T cells correlates with poor prognosis in MM through IL-22 and IL-13 protumor activity and suggest that interference with IL-22 and IL-13 signaling pathways could be exploited for therapeutic intervention.
Keywords: Ab, antibody; BM, bone marrow; BMMCs, bone marrow mononuclear cells; DCs, dendritic cells; Dx, dexamethasone; ICS, intracellular cytokine staining; IFN, interferon; IL, interleukin; ISS, International Staging System; LCL, Epstein–Barr virus-transformed B lymphoblastoid cell line; Ln, lenalidomide; MGUS, monoclonal gammopathy of undetermined clinical significance; MM, multiple myeloma; MSC, mesenchymal stromal cell; PB, peripheral blood; PBMCs, peripheral blood mononuclear cells; pDCs, plasmacytoid dendritic cells; SMM, smoldering multiple myeloma; Th, T helper; TNF, tumor necrosis factor; Treg, regulatory T cells; WB, Western blot; CD4+ T helper lymphocytes; IL-22RA1; Th22 cells; bone marrow mesenchymal stromal cells; bone marrow microenvironment; interleukin-13; interleukin-22; multiple myeloma.
Figures
References
-
- Palumbo A, Anderson K. Multiple myeloma. N Engl J Med 2011; 364:1046-60; PMID:; http://dx.doi.org/10.1056/NEJMra1011442 - DOI - PubMed
-
- Hideshima T, Mitsiades C, Tonon G, Richardson PG, Anderson KC. Understanding multiple myeloma pathogenesis in the bone marrow to identify new therapeutic targets. Nat Rev Cancer 2007; 7:585-98; PMID:; http://dx.doi.org/10.1038/nrc2189 - DOI - PubMed
-
- Dimopoulos MA, San-Miguel JF, Anderson KC. Emerging therapies for the treatment of relapsed or refractory multiple myeloma. Eur J Haematol 2011; 86:1-15; PMID:; http://dx.doi.org/10.1111/j.1600-0609.2010.01542.x - DOI - PubMed
-
- Borrello I. Can we change the disease biology of multiple myeloma? Leuk Res 2012; 36(Suppl 1):S3-12; PMID:; http://dx.doi.org/10.1016/S0145-2126(12)70003-6 - DOI - PMC - PubMed
-
- Rajkumar SV. Treatment of multiple myeloma. Nat Rev Clin Oncol 2011; 8:479-91; PMID:; http://dx.doi.org/10.1038/nrclinonc.2011.63 - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous