

Computational Psychiatry: towards a mathematically informed understanding of mental illness
- PMID: 26157034
- PMCID: PMC4717449
- DOI: 10.1136/jnnp-2015-310737
Computational Psychiatry: towards a mathematically informed understanding of mental illness
Abstract
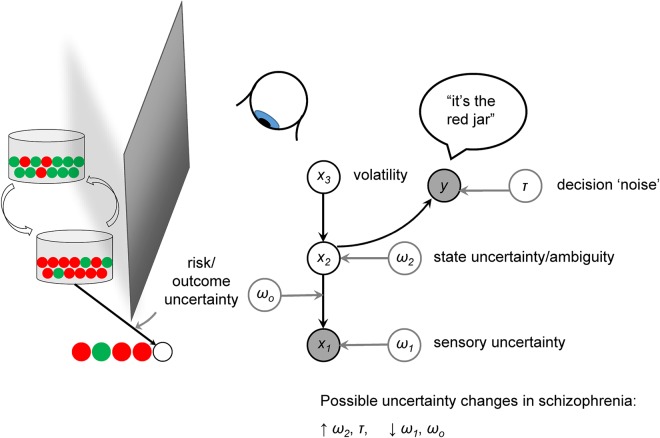
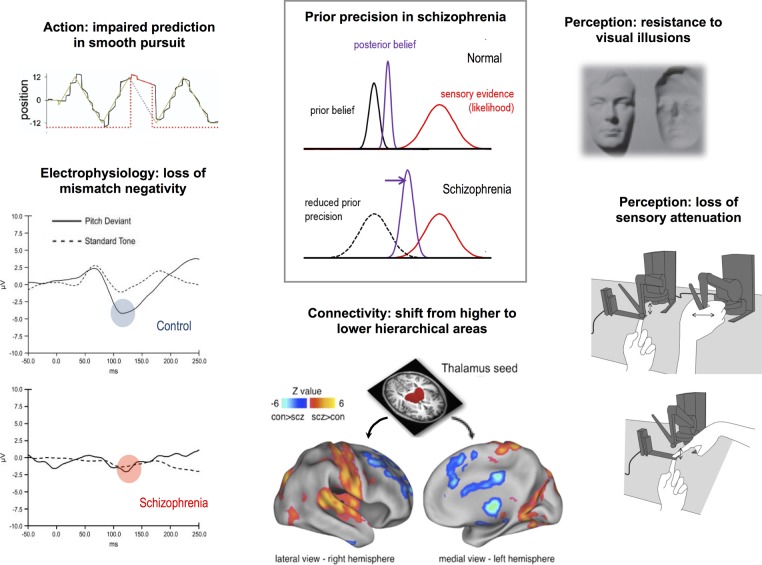
Computational Psychiatry aims to describe the relationship between the brain's neurobiology, its environment and mental symptoms in computational terms. In so doing, it may improve psychiatric classification and the diagnosis and treatment of mental illness. It can unite many levels of description in a mechanistic and rigorous fashion, while avoiding biological reductionism and artificial categorisation. We describe how computational models of cognition can infer the current state of the environment and weigh up future actions, and how these models provide new perspectives on two example disorders, depression and schizophrenia. Reinforcement learning describes how the brain can choose and value courses of actions according to their long-term future value. Some depressive symptoms may result from aberrant valuations, which could arise from prior beliefs about the loss of agency ('helplessness'), or from an inability to inhibit the mental exploration of aversive events. Predictive coding explains how the brain might perform Bayesian inference about the state of its environment by combining sensory data with prior beliefs, each weighted according to their certainty (or precision). Several cortical abnormalities in schizophrenia might reduce precision at higher levels of the inferential hierarchy, biasing inference towards sensory data and away from prior beliefs. We discuss whether striatal hyperdopaminergia might have an adaptive function in this context, and also how reinforcement learning and incentive salience models may shed light on the disorder. Finally, we review some of Computational Psychiatry's applications to neurological disorders, such as Parkinson's disease, and some pitfalls to avoid when applying its methods.
Keywords: COGNITION; DEPRESSION; PSYCHIATRY; PSYCHOPHARMACOLOGY; SCHIZOPHRENIA.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
References
-
- American Psychiatric Association. DSM 5. American Psychiatric Association, 2013.
-
- World Health Organization. ICD-10: International classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. Geneva: WHO, 1992.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical