

Usefulness of human epididymis protein 4 in predicting cytoreductive surgical outcomes for advanced ovarian tubal and peritoneal carcinoma
- PMID: 26157328
- PMCID: PMC4490196
- DOI: 10.3978/j.issn.1000-9604.2015.06.01
Usefulness of human epididymis protein 4 in predicting cytoreductive surgical outcomes for advanced ovarian tubal and peritoneal carcinoma
Abstract
Objective: Human epididymis protein 4 (HE4) is a promising biomarker of epithelial ovarian cancer (EOC). But its role in assessing the primary optimal debulking (OD) of EOC remains unknown. The purpose of this study is to elucidate the ability of preoperative HE4 in predicting the primary cytoreductive outcomes in advanced EOC, tubal or peritoneal carcinoma.
Methods: We reviewed the records of 90 patients with advanced ovarian, tubal or peritoneal carcinoma who underwent primary cytoreduction at the Department of Obstetrics and Gynecology of Peking University People's Hospital between November 2005 and October 2010. Preoperative serum HE4 and CA125 levels were detected with EIA kit. A receiver operating characteristic (ROC) curve was used to determine the most useful HE4 cut-off value. Logistic regression analysis was performed to identify significant preoperative clinical characteristics to predict optimal primary cytoreduction.
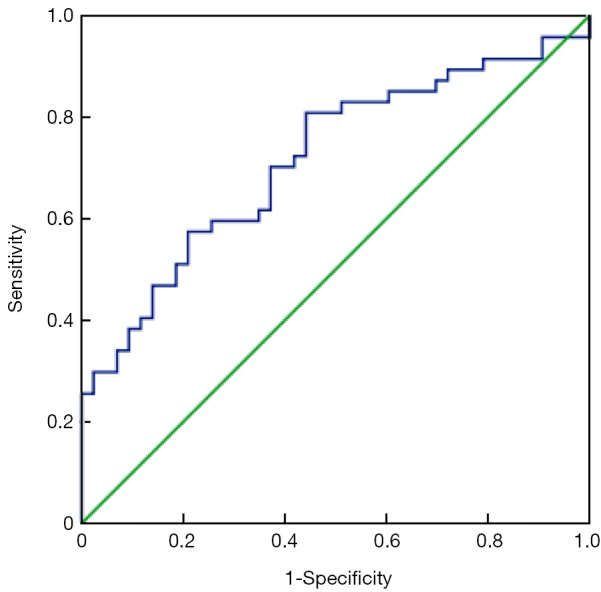
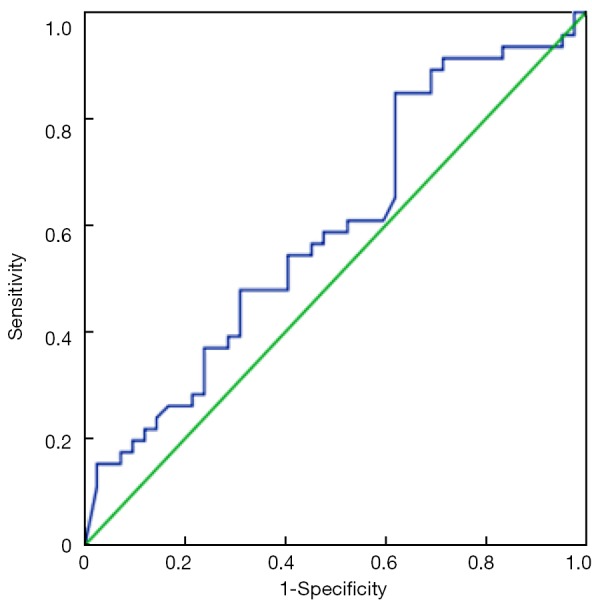
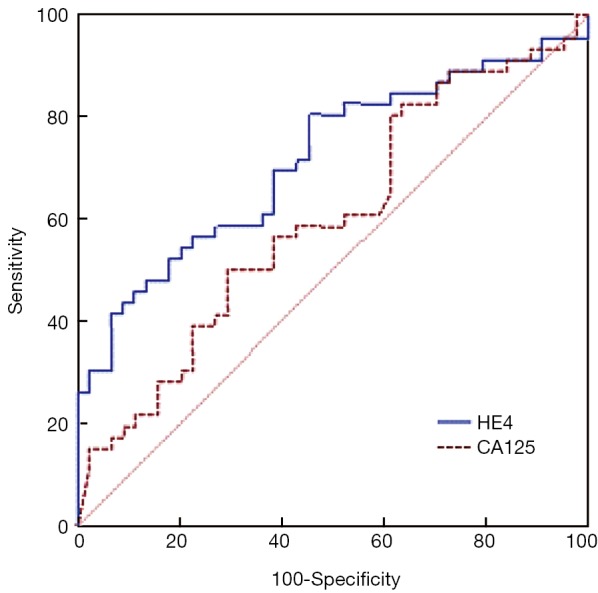
Results: OD was achieved in 47.7% (43/48) of patients. The median preoperative HE4 level for patients with OD vs. suboptimal debulking was 423 and 820 pmol/L, respectively (P<0.001). The areas under the ROC curve for HE4 and CA125 were 0.716 and 0.599, respectively (P=0.080). The most useful HE4 cut-off value was 473 pmol/L. Suboptimal cytoreduction was obtained in 66.7% (38/57) of cases with HE4 ≥473 pmol/L compared with only 27.3% (9/33) of cases with HE4 <473 pmol/L. At this threshold, the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) for diagnosing suboptimal debulking were 81%, 56%, 67%, and 73%, respectively. Logistic regression analysis showed that the patients with HE4 ≥473 pmol/L were less likely to achieve OD (odds ratio =5.044, P=0.002).
Conclusions: Preoperative serum HE4 may be helpful to predict whether optimal cytoreductive surgery could be obtained or whether extended cytoreduction would be needed by an interdisciplinary team.
Keywords: CA125; Human epididymis protein 4 (HE4); advanced epithelial ovarian cancer (EOC); optimal cytoreduction.
Figures
References
-
- International Agency for Research on Cancer. GLOBOCAN 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012. Accessed in 2015. Available online: http://globocan.iarc.fr/Pages/fact_sheets_population.aspx
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin 2008;58:71-96. - PubMed
-
- Bristow RE, Tomacruz RS, Armstrong DK, et al. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol 2002;20:1248-59. - PubMed
-
- Peiretti M, Zanagnolo V, Aletti GD, et al. Role of maximal primary cytoreductive surgery in patients with advanced epithelial ovarian and tubal cancer: Surgical and oncological outcomes. Single institution experience. Gynecol Oncol 2010;119:259-64. - PubMed
-
- Chi DS, Venkatraman ES, Masson V, et al. The ability of preoperative serum CA-125 to predict optimal primary tumor cytoreduction in stage III epithelial ovarian carcinoma. Gynecol Oncol 2000;77:227-31. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous