

Dynamic behavior of venous collapsibility and central venous pressure during standardized crystalloid bolus: A prospective, observational, pilot study
- PMID: 26157649
- PMCID: PMC4477400
- DOI: 10.4103/2229-5151.158392
Dynamic behavior of venous collapsibility and central venous pressure during standardized crystalloid bolus: A prospective, observational, pilot study
Abstract
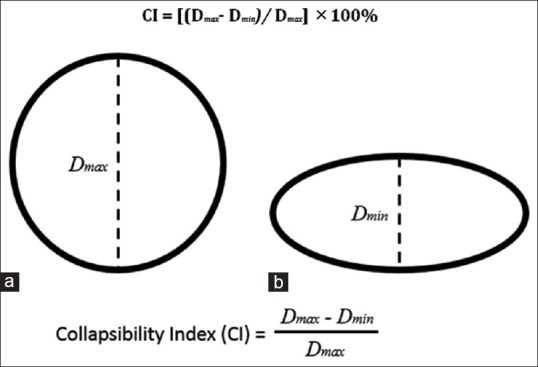
Introduction: Measurement of intravascular volume status is an ongoing challenge for physicians in the surgical intensive care unit (SICU). Most surrogates for volume status, including central venous pressure (CVP) and pulmonary artery wedge pressure, require invasive lines associated with a number of potential complications. Sonographic assessment of the collapsibility of the inferior vena cava (IVC) has been described as a noninvasive method for determining volume status. The purpose of this study was to analyze the dynamic response in IVC collapsibility index (IVC-CI) to changes in CVP in SICU patients receiving fluid boluses for volume resuscitation.
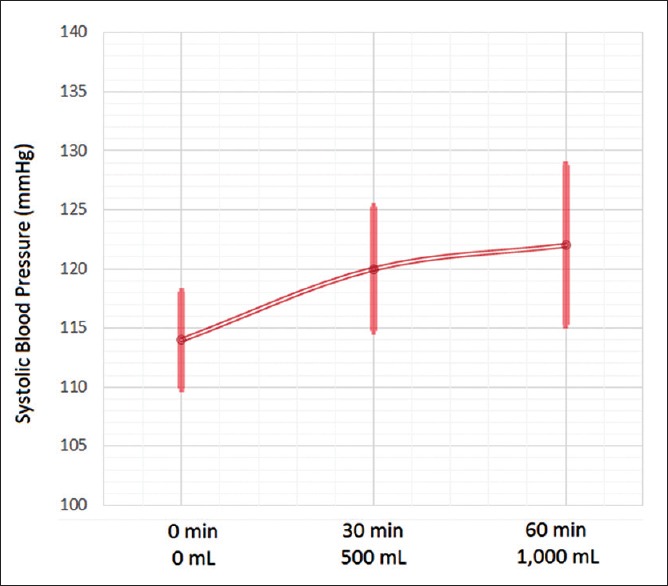
Materials and methods: A prospective pilot study was conducted on a sample of SICU patients who met clinical indications for intravenous (IV) fluid bolus and who had preexisting central venous access. Boluses were standardized to crystalloid administration of either 500 mL over 30 min or 1,000 mL over 60 min, as clinically indicated. Concurrent measurements of venous CI (VCI) and CVP were conducted right before initiation of IV bolus (i.e. time 0) and then at 30 and 60 min (as applicable) after bolus initiation. Patient demographics, ventilatory parameters, and vital sign assessments were recorded, with descriptive outcomes reported due to the limited sample size.
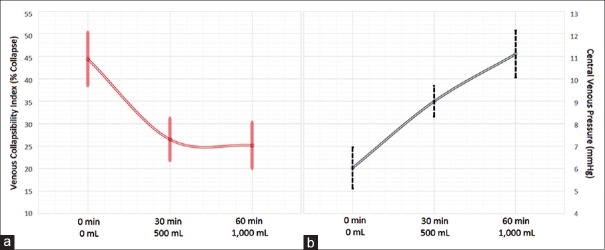
Results: Twenty patients received a total of 24 IV fluid boluses. There were five recorded 500 mL boluses given over 30 min and 19 recorded 1,000 mL boluses given over 60 min. Mean (median) CVP measured at 0, 30, and 60 minutes post-bolus were 6.04 ± 3.32 (6.5), 9.00 ± 3.41 (8.0), and 11.1 ± 3.91 (12.0) mmHg, respectively. Mean (median) IVC-CI values at 0, 30, and 60 min were 44.4 ± 25.2 (36.5), 26.5 ± 22.8 (15.6), and 25.2 ± 21.2 (14.8), respectively.
Conclusions: Observable changes in both VCI and CVP are apparent during an infusion of a standardized fluid bolus. Dynamic changes in VCI as a measurement of responsiveness to fluid bolus are inversely related to changes seen in CVP. Moreover, an IV bolus tends to produce an early response in VCI, while the CVP response is more gradual. Given the noninvasive nature of the measurement technique, VCI shows promise as a method of dynamically measuring patient response to fluid resuscitation. Further studies with larger sample sizes are warranted.
Keywords: Central venous pressure; Point-of-care ultrasound; inferior vena cava collapsibility index; intravascular volume status assessment; intravenous fluid bolus.
Conflict of interest statement
Figures
Similar articles
-
Prospective evaluation of intravascular volume status in critically ill patients: does inferior vena cava collapsibility correlate with central venous pressure?J Trauma Acute Care Surg. 2014 Apr;76(4):956-63; discussion 963-4. doi: 10.1097/TA.0000000000000152. J Trauma Acute Care Surg. 2014. PMID: 24662857
-
Comparison of inferior vena cava collapsibility and central venous pressure in assessing volume status in shocked patients.Afr J Emerg Med. 2022 Sep;12(3):165-171. doi: 10.1016/j.afjem.2022.04.005. Epub 2022 May 17. Afr J Emerg Med. 2022. PMID: 35599841 Free PMC article.
-
Sonographic evaluation of intravascular volume status in the surgical intensive care unit: a prospective comparison of subclavian vein and inferior vena cava collapsibility index.J Surg Res. 2013 Sep;184(1):561-6. doi: 10.1016/j.jss.2013.05.040. Epub 2013 Jun 3. J Surg Res. 2013. PMID: 23764308 Clinical Trial.
-
The efficacy of sonographic measurement of inferior vena cava diameter as an estimate of central venous pressure.Cardiovasc Ultrasound. 2016 Aug 20;14(1):33. doi: 10.1186/s12947-016-0076-1. Cardiovasc Ultrasound. 2016. PMID: 27542597 Free PMC article. Review.
-
Usefulness of Non-Invasive Parameters (Inferior Vena Cava Diameter, Inferior Vena Cava Collapsibility, Inferior Vena Cava-Aortic Ratio) for Hemodynamic Monitoring in Critically Ill Children: A Systematic Review.Med Devices (Auckl). 2024 Mar 18;17:123-133. doi: 10.2147/MDER.S454849. eCollection 2024. Med Devices (Auckl). 2024. PMID: 38525306 Free PMC article. Review.
Cited by
-
Correlations between pulmonary artery pressures and inferior vena cava collapsibility in critically ill surgical patients: An exploratory study.Int J Crit Illn Inj Sci. 2016 Oct-Dec;6(4):194-199. doi: 10.4103/2229-5151.195449. Int J Crit Illn Inj Sci. 2016. PMID: 28149825 Free PMC article.
-
Keys to successful organ procurement: An experience-based review of clinical practices at a high-performing health-care organization.Int J Crit Illn Inj Sci. 2017 Apr-Jun;7(2):91-100. doi: 10.4103/IJCIIS.IJCIIS_30_17. Int J Crit Illn Inj Sci. 2017. PMID: 28660162 Free PMC article. Review.
-
Role of the inferior vena cava collapsibility index in predicting propofol-induced hypotension in patients undergoing colonoscopy.BMC Anesthesiol. 2025 Feb 14;25(1):73. doi: 10.1186/s12871-025-02945-y. BMC Anesthesiol. 2025. PMID: 39953383 Free PMC article.
-
Inferior vena cava diameter as a guide in hypotensive patients for appropriate saline therapy: An observational study.Int J Crit Illn Inj Sci. 2018 Jul-Sep;8(3):160-164. doi: 10.4103/IJCIIS.IJCIIS_27_18. Int J Crit Illn Inj Sci. 2018. PMID: 30181974 Free PMC article.
-
Advancing clinician-performed sonography in the twenty-first century: building on the rich legacy of the twentieth century pioneers.Eur J Trauma Emerg Surg. 2016 Apr;42(2):115-8. doi: 10.1007/s00068-016-0652-y. Epub 2016 Mar 4. Eur J Trauma Emerg Surg. 2016. PMID: 26942742 No abstract available.
References
-
- Evans DC, Doraiswamy VA, Prosciak MP, Silviera M, Seamon MJ, Rodriguez Funes V, et al. Complications associated with pulmonary artery catheters: A comprehensive clinical review. Scand J Surg. 2009;98:199–208. - PubMed
-
- Patel C, Laboy V, Venus B, Mathru M, Wier D. Acute complications of pulmonary artery catheter insertion in critically ill patients. Crit Care Med. 1986;14:195–7. - PubMed
-
- Stawicki SP, Adkins EJ, Eiferman DS, Evans DC, Ali NA, Njoku C, et al. Prospective evaluation of intravascular volume status in critically ill patients: Does inferior vena cava collapsibility correlate with central venous pressure? J Trauma Acute Care Surg. 2014;76:956–63. - PubMed
-
- Stawicki SP, Braslow BM, Panebianco NL, Kirkpatrick JN, Gracias VH, Hayden GE, et al. Intensivist use of hand-carried ultrasonography to measure IVC collapsibility in estimating intravascular volume status: Correlations with CVP. J Am Coll Surg. 2009;209:55–61. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
