

Case Reports
doi: 10.14309/crj.2013.14.
eCollection 2013 Oct.
Giant Inflammatory Fibroid Polyp of the Descending Colon Treated with Endoscopic Resection
Affiliations
- PMID: 26157816
- PMCID: PMC4435274
- DOI: 10.14309/crj.2013.14
Item in Clipboard
Case Reports
Giant Inflammatory Fibroid Polyp of the Descending Colon Treated with Endoscopic Resection
ACG Case Rep J.
.
Abstract
Inflammatory fibroid polyps (IFPs) of the colon are very rare, reactive, non-neoplastic polyps that may grow to large sizes but do not carry any risk of malignancy. Because of their size, IFPs are usually treated with surgery; however, size alone should not be an indication for surgery. Depending on the location and morphology of the polyp, endoscopic resection should be considered. We here describe a case of a giant IFP that was successfully removed with endoscopy without complication or recurrence.
Figures
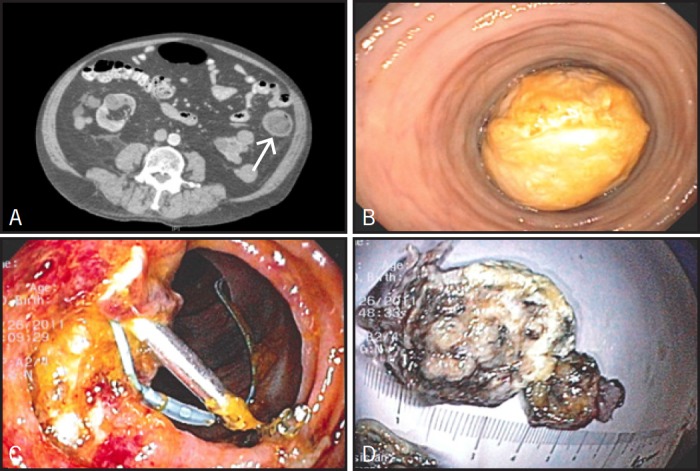
(A) CT scan showing large hypodense hetereogenous mass measuring 5 cm (arrow), occupying most of the descending colon. (B) Endoscopic view of the large colonic mass obstructing the lumen of the descending colon. (C) Endoscopic view of the post polypectomy site (endoloop and endoclips seen at the site). (D) Gross view of the colonic mass after endoscopic resection.
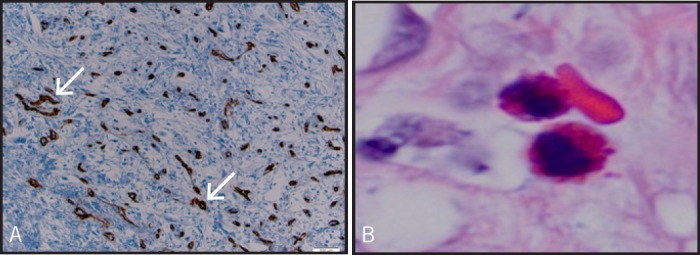
(A) Intermediate power view of the inflammatory fibroid polyp showing the rich vascular supply (arrows) highlighted by a CD34 immunostain. Tissue section. CD 34 immunostain. Original magnification ×100. (B) Eosinophils within the stroma. Inflammatory fibroid polyp. Tissue section, hematoxylin, and eosin; original magnification ×1,000.
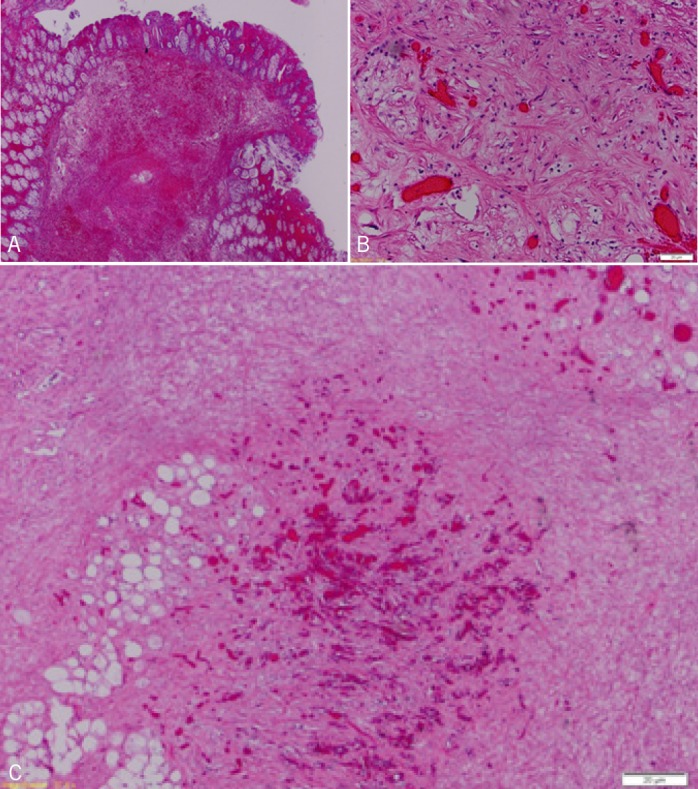
(A) Low power view. Submucosal stromal proliferation with superimposed hemorrhage. Inflammatory fibroid polyp, tissue section. Hematoxylin and eosin, original magnification ×20. (B) High power view of the inflammatory fibroid polyp displaying a rich vascularized area with branching capillaries surrounded by a collagenous stroma containing bland spindle cells. Tissue section. Hematoxylin and eosin, original magnification ×200. (C) Low power view of the deep aspect of the inflammatory fibroid polyp displaying rich vascularized areas. Tissue section. Hematoxylin and eosin, original magnification ×40.
Similar articles
-
Giant Inflammatory Fibroid Polyp of the Hepatic Flexure of Colon Presenting with an Acute Abdomen.Case Rep Gastrointest Med. 2016;2016:2178639. doi: 10.1155/2016/2178639. Epub 2016 Oct 3. Case Rep Gastrointest Med. 2016. PMID: 27781129 Free PMC article.
-
Unusual presentation of a giant benign inflammatory polyp in the upper esophagus.Int J Surg Case Rep. 2015;6C:206-9. doi: 10.1016/j.ijscr.2014.12.013. Epub 2014 Dec 19. Int J Surg Case Rep. 2015. PMID: 25544491 Free PMC article.
-
Gastric inflammatory fibroid polyp tumor with acute intestinal obstruction-Vanek's tumor can mimick a giant gastrointestinal stromal tumor or a gastric lymphoma.J Vis Surg. 2018 Mar 16;4:54. doi: 10.21037/jovs.2018.02.09. eCollection 2018. J Vis Surg. 2018. PMID: 29682464 Free PMC article.
-
Experience in the endoscopic management of large colonic polyps.ANZ J Surg. 2003 Dec;73(12):988-95. doi: 10.1046/j.1445-2197.2003.t01-23-.x. ANZ J Surg. 2003. PMID: 14632888 Review.
-
Invasive inflammatory fibroid polyp of the stomach: a case report and literature review.BMC Gastroenterol. 2018 May 31;18(1):74. doi: 10.1186/s12876-018-0808-9. BMC Gastroenterol. 2018. PMID: 29855265 Free PMC article. Review.
Cited by
-
Giant Inflammatory Fibroid Polyp of the Hepatic Flexure of Colon Presenting with an Acute Abdomen.Case Rep Gastrointest Med. 2016;2016:2178639. doi: 10.1155/2016/2178639. Epub 2016 Oct 3. Case Rep Gastrointest Med. 2016. PMID: 27781129 Free PMC article.
-
Inflammatory Fibroid Polyp of the Gastrointestinal Tract: A Systematic Review for a Benign Tumor.In Vivo. 2021 Jan-Feb;35(1):81-93. doi: 10.21873/invivo.12235. In Vivo. 2021. PMID: 33402453 Free PMC article.
-
Masquerading in the midgut: a rare diagnosis in a patient with recurrent abdominal pain.Frontline Gastroenterol. 2019 Jun 27;11(5):420-422. doi: 10.1136/flgastro-2019-101222. eCollection 2020. Frontline Gastroenterol. 2019. PMID: 32879725 Free PMC article.
-
Two Cases of Leiomyoma in the Colon Masquerading as Other Types of Colonic Pedunculated Polyps.Case Rep Gastrointest Med. 2018 Apr 29;2018:8272313. doi: 10.1155/2018/8272313. eCollection 2018. Case Rep Gastrointest Med. 2018. PMID: 29854494 Free PMC article.
-
Giant Ileocecal Inflammatory Fibroid Polyp: Unique Clinical Presentation.Case Rep Surg. 2020 Jul 21;2020:8811404. doi: 10.1155/2020/8811404. eCollection 2020. Case Rep Surg. 2020. PMID: 32774977 Free PMC article.
References
-
- Matsushita M, Hajiro K, Okazaki K, Takakuwa H. Gastric inflammatory fibroid polyps: Endoscopic ultrasonographic analysis in comparison with the histology. Gastrointest Endosc. 1997;46(1):53–7. - PubMed
-
- Sakamoto T, Kato H, Okabe T, et al. . A large inflammatory fibroid polyp of the colon treated by endoclip-assisted endoscopic polypectomy. Dig Liver Dis. 2005;37(12):968–72. - PubMed
-
- Konjetzny GE. Uber magenfibrome. Beitr Klin Chir. 1920;119:53–61.
-
- Kofler E. Uber die granulome des magen-darmashlauches. Virchows Arch. 1952;321(2):121–33. - PubMed
-
- Helwig EB, Ranier A. Inflammatory fibroid polyps of the stomach. Surg Gynecol Obstet. 1953;96(3):335–67. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
