

Leydig cell tumor in a patient with 49,XXXXY karyotype: a review of literature
- PMID: 26160035
- PMCID: PMC4496935
- DOI: 10.1186/s12958-015-0071-7
Leydig cell tumor in a patient with 49,XXXXY karyotype: a review of literature
Abstract
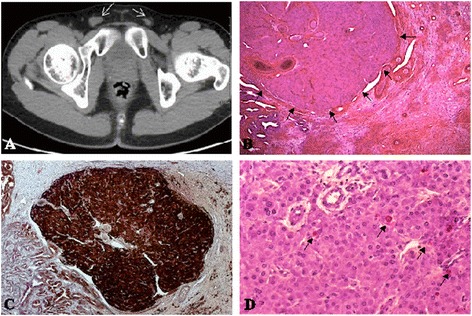
49,XXXXY pentasomy or Fraccaro's syndrome is the most severe variant of Klinefelter's syndrome (KS) affecting about 1/85000 male births. The classical presentation is the triad: mental retardation, hypergonadotropic hypogonadism and radio ulnar synostosis. Indeed, the reproductive function of Fraccaro's syndrome is distinguished from KS. Besides, Leydig cell tumors are described in cases of KS, but never documented in the Klinefelter variants.We describe a young adult of 22 years old who presented with hyper gonadotropic hypogonadism, delayed puberty and bilateral micro-cryptorchidism. Chromosomal pentasomy was confirmed since infancy. Bilateral orchidectomy revealed a unilateral well-circumscribed Leydig cell tumor associated with bilateral Leydig cell hyperplasia.Inspired from reporting the first case of Leydig cell tumor in a 49,XXXXY patient, we summarize the particularities of testicular function in 49,XXXXY from one side, and the risk and mechanisms of Leydig cell tumorigenesis in Klinefelter variants on the other side. The histological destructions in 49,XXXXY testes and hypogonadism are more profound than in Klinefelter patients, with early Sertoli, Leydig and germ cell destruction. Furthermore, the risk of Leydigioma development in KS and its variants remains a dilemma. We believe that the risk of Leydigioma is much higher in KS than the general population. By contrast, the risk could be lower in the Klinefelter variants with more than 3 supplementary X chromosomes, owing to an earlier and more profound destruction of Leydig cells rendering them irresponsive to chronic Luteinizing hormone (LH) stimulation.
Figures
References
-
- Linden MG, Bender BG, Robinson A. Sex chromosome tetrasomy and pentasomy. Pediatrics. 1995;96(4 Pt 1):672–682. - PubMed
-
- Klinefelter HF, Reifenstein EC, Albright F. Syndrome characterized by gynecomastia, aspermatogenesis without A-Leydigism, and increased excretion of follicle-stimulating hormone1. J Clin Endocrinol Metab. 1942;2:615–627.
-
- Fromantin M, Pesquies P, Serrurier B, Gautier D, Canivet B, Grenier J, Scholler R. Klinefelter’s syndrome in 19 year old adolescents. (100 cases detected during selection for National Service) Ann Méd Interne. 1977;128:239–244. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
