

Exploratory cost-effectiveness analysis of cardiac resynchronization therapy with systematic device optimization vs. standard (non-systematic) optimization: a multinational economic evaluation
- PMID: 26160650
- PMCID: PMC4498000
- DOI: 10.1186/s13561-015-0057-3
Exploratory cost-effectiveness analysis of cardiac resynchronization therapy with systematic device optimization vs. standard (non-systematic) optimization: a multinational economic evaluation
Abstract
Background: Recent studies provide evidence of improved clinical benefits associated with cardiac resynchronization therapy (CRT) optimization. Our analysis explores the cost-effectiveness of systematically optimized (SO, 3 times a year) vs. non-systematically optimized (NSO, less than 3 times a year) CRT, whatever the echo optimization method used (manual or SonR® automatic). A longitudinal cohort model was developed to predict clinical and economic outcomes for SO vs. NSO strategies over 5 years. The analysis was performed from the payer perspective. Data from CLEAR study post-hoc analysis was used with 199 pts with CRT pacemaker (CRT-P). The main economic outcome measure was incremental cost-effectiveness (ICER) expressed as cost per Quality Adjusted Life Years (QALY) gained. To assess the impact of data uncertainty, a sensitivity analysis was performed. The model also predicts outcomes for the two optimization strategies for CRT-D therapy vs. optimal medical treatment (OPT).
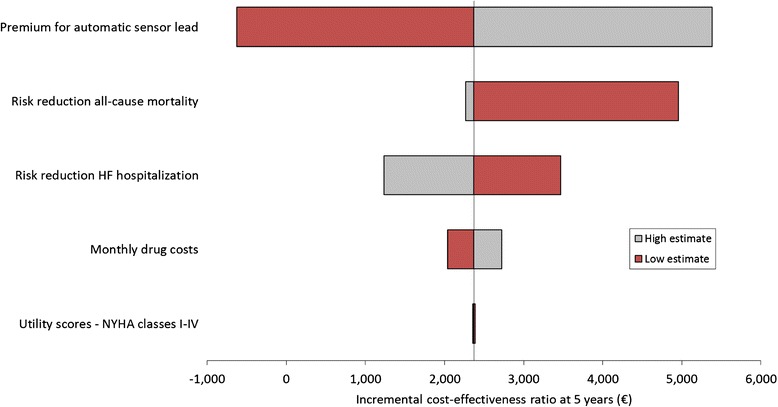
Results: At 1 year, ICERs for SO CRT vs. NSO CRT-P range between <euro> 22,226 (Spain) and <euro> 26,977 (Italy). Therefore, on the basis of a Willingness-To-Pay of <euro>30,000 per QALY, the SO method develops into a cost effective strategy from 1 year, onwards. These favorable outcomes are supported by the sensitivity analysis. Systematic optimization of CRT-D might also improve the cost-effectiveness of this device therapy by 27 % to 30 % dependent on the country analyzed, at 5 years.
Conclusions: Our economic evaluation shows promising health economic benefits associated with SO CRT. These preliminary findings need further confirmation.
Figures



References
-
- López-Sendón J. The heart failure epidemic. Medicographia. 2011;4:363–369.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
