

Racial Differences in BRAF/KRAS Mutation Rates and Survival in Stage III Colon Cancer Patients
- PMID: 26160882
- PMCID: PMC5758035
- DOI: 10.1093/jnci/djv186
Racial Differences in BRAF/KRAS Mutation Rates and Survival in Stage III Colon Cancer Patients
Abstract
Background: It is unknown if, after controlling for clinicopathologic variables and treatment, racial disparities in colon cancer outcomes persist. Molecular marker analysis in North American patients comparing Asians with other races has not been reported.
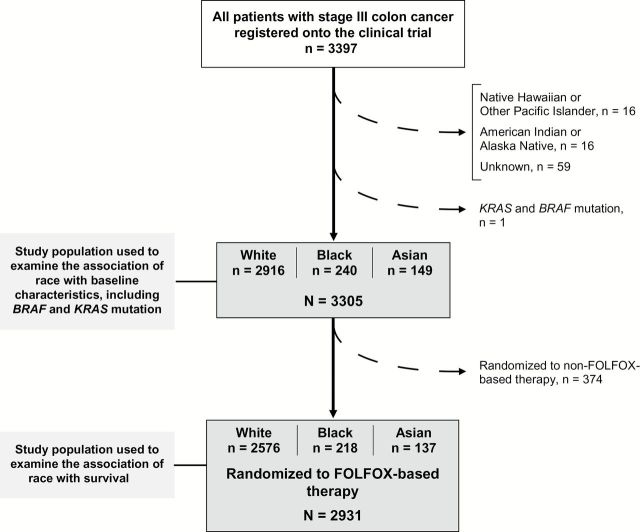
Methods: BRAF (V600E) and KRAS mutations were analyzed in node-positive colon cancer patients (n = 3305) treated with FOLFOX-based chemotherapy in an adjuvant trial (Alliance N0147). Race categories included Asian, black, or white. Cox models were used to estimate disease-free survival (DFS) and time to recurrence (TTR). All statistical tests were two-sided.
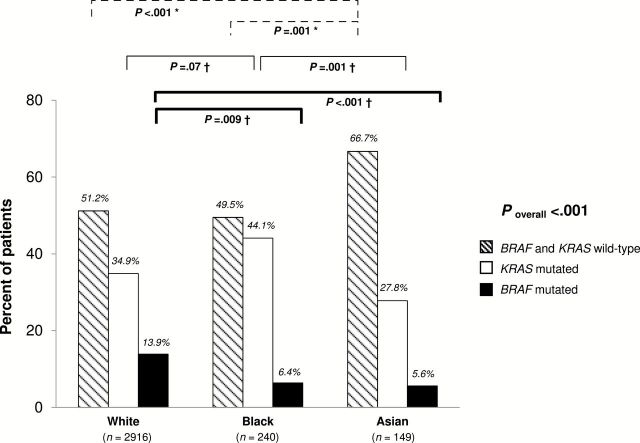
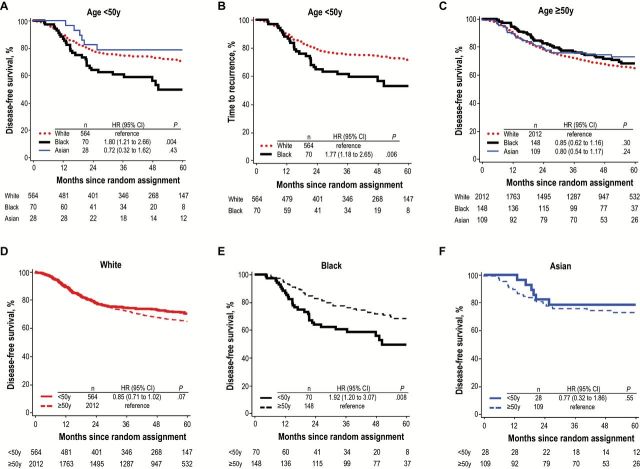
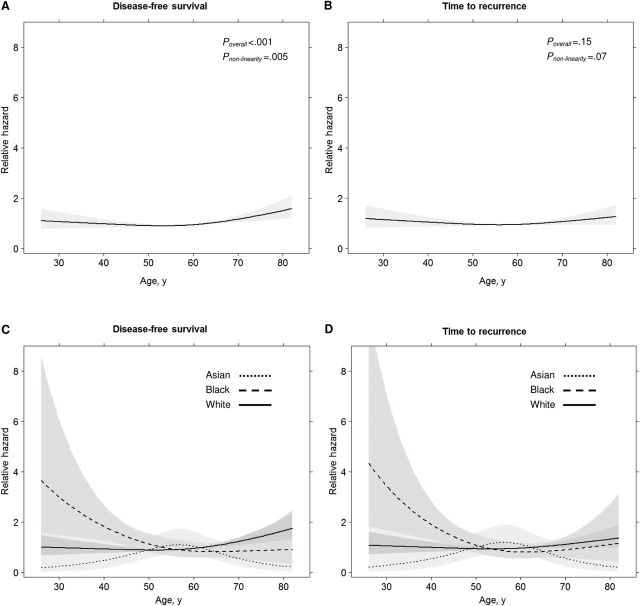
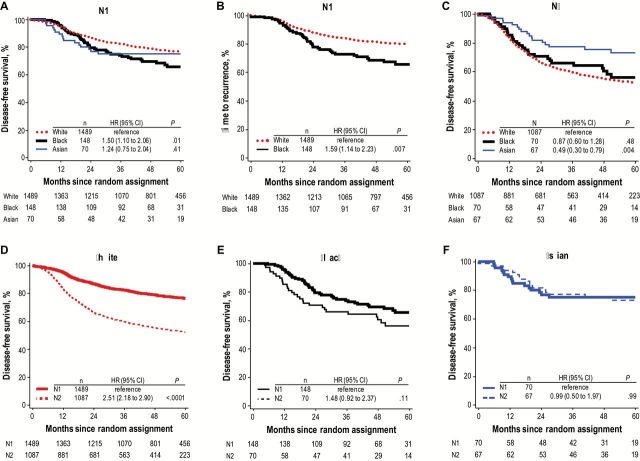
Results: BRAF mutation frequency in tumors from whites (13.9%) was twice that of tumors from Asians or blacks. KRAS mutation rates were highest in tumors from blacks (44.1%). KRAS/BRAF wild-type tumors were most common among Asians (66.7%) (P overall < .001). The prognostic impact of race differed by age and N stage (both P interaction < .02). Compared with whites, blacks had shorter DFS among patients younger than age 50 years (hazard ratio [HR] = 2.84, 95% confidence interval [CI] = 1.73 to 4.66) or with N1 disease (HR = 1.54, 95% CI = 1.04 to 2.29), independent of BRAF, KRAS, and other covariates. Findings were consistent using TTR as the outcome. Asians had longer DFS among N2 tumors that was partly mediated by less frequent BRAF mutation.
Conclusions: Colon cancers from Asians have a lower rate of BRAF and KRAS mutations than blacks or whites. We report a novel interaction of race with age and N stage in node-positive disease, indicating that racial disparities in survival persist despite uniform stage and treatment in a phase III trial.
© The Author 2015. Published by Oxford University Press. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Molecular markers identify subtypes of stage III colon cancer associated with patient outcomes.Gastroenterology. 2015 Jan;148(1):88-99. doi: 10.1053/j.gastro.2014.09.041. Epub 2014 Oct 8. Gastroenterology. 2015. PMID: 25305506 Free PMC article. Clinical Trial.
-
Association of DNA Mismatch Repair and Mutations in BRAF and KRAS With Survival After Recurrence in Stage III Colon Cancers : A Secondary Analysis of 2 Randomized Clinical Trials.JAMA Oncol. 2017 Apr 1;3(4):472-480. doi: 10.1001/jamaoncol.2016.5469. JAMA Oncol. 2017. PMID: 28006055 Free PMC article. Clinical Trial.
-
KRAS codon 12 and 13 mutations in relation to disease-free survival in BRAF-wild-type stage III colon cancers from an adjuvant chemotherapy trial (N0147 alliance).Clin Cancer Res. 2014 Jun 1;20(11):3033-43. doi: 10.1158/1078-0432.CCR-13-3140. Epub 2014 Mar 31. Clin Cancer Res. 2014. PMID: 24687927 Free PMC article. Clinical Trial.
-
KRAS and BRAF Mutations in Stage II and III Colon Cancer: A Systematic Review and Meta-Analysis.J Natl Cancer Inst. 2022 Apr 11;114(4):517-527. doi: 10.1093/jnci/djab190. J Natl Cancer Inst. 2022. PMID: 34542636 Free PMC article.
-
The prognostic value of KRAS and BRAF in stage I-III colorectal cancer. A systematic review.Ann Ital Chir. 2019;90:127-137. Ann Ital Chir. 2019. PMID: 30739887
Cited by
-
American Indian/Alaska Native and black colon cancer patients have poorer cause-specific survival based on disease stage and anatomic site of diagnosis.Cancer Epidemiol. 2022 Oct;80:102229. doi: 10.1016/j.canep.2022.102229. Epub 2022 Jul 21. Cancer Epidemiol. 2022. PMID: 35872382 Free PMC article.
-
Prevalence of the BRAF p.v600e variant in patients with colorectal cancer from Mexico and its estimated frequency in Latin American and Caribbean populations.J Investig Med. 2020 Jun;68(5):985-991. doi: 10.1136/jim-2020-001301. Epub 2020 Mar 16. J Investig Med. 2020. PMID: 32184228 Free PMC article.
-
The molecular heterogeneity of sporadic colorectal cancer with different tumor sites in Chinese patients.Oncotarget. 2017 Jul 25;8(30):49076-49083. doi: 10.18632/oncotarget.16176. Oncotarget. 2017. PMID: 28416767 Free PMC article.
-
An overview of cancer health disparities: new approaches and insights and why they matter.Carcinogenesis. 2021 Feb 11;42(1):2-13. doi: 10.1093/carcin/bgaa121. Carcinogenesis. 2021. PMID: 33185680 Free PMC article. Review.
-
Clinical Significance of Somatic Mutations in RAS/RAF/MAPK Signaling Pathway in Moroccan and North African Colorectal Cancer Patients.Asian Pac J Cancer Prev. 2022 Nov 1;23(11):3725-3733. doi: 10.31557/APJCP.2022.23.11.3725. Asian Pac J Cancer Prev. 2022. PMID: 36444585 Free PMC article.
References
-
- Center MM, Jemal A, Ward E. International trends in colorectal cancer incidence rates. Cancer Epidemiol Biomarkers Prev. 2009;18(6):1688–1694. - PubMed
-
- Umar A, Greenwald P. Alarming colorectal cancer incidence trends: a case for early detection and prevention. Cancer Epidemiol Biomarkers Prev. 2009;18(6):1672–1673. - PubMed
-
- Robbins AS, Siegel RL, Jemal A. Racial disparities in stage-specific colorectal cancer mortality rates from 1985 to 2008. J Clin Oncol. 2012;30(4):401–405. - PubMed
-
- Polite BN, Dignam JJ, Olopade OI. Colorectal cancer model of health disparities: understanding mortality differences in minority populations. J Clin Oncol. 2006;24(14):2179–2187. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- CA-37404/CA/NCI NIH HHS/United States
- K05CA-142885/CA/NCI NIH HHS/United States
- U10 CA037404/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- U24 CA114740/CA/NCI NIH HHS/United States
- CA-25224/CA/NCI NIH HHS/United States
- U10CA180882/CA/NCI NIH HHS/United States
- U10 CA180850/CA/NCI NIH HHS/United States
- UG1 CA232760/CA/NCI NIH HHS/United States
- UG1 CA189823/CA/NCI NIH HHS/United States
- U10 CA180790/CA/NCI NIH HHS/United States
- U10 CA180882/CA/NCI NIH HHS/United States
- U10CA180821/CA/NCI NIH HHS/United States
- K05 CA142885/CA/NCI NIH HHS/United States
- U10 CA025224/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
