

Improving Quality and Potency Testing for Umbilical Cord Blood: A New Perspective
- PMID: 26160959
- PMCID: PMC4542872
- DOI: 10.5966/sctm.2015-0036
Improving Quality and Potency Testing for Umbilical Cord Blood: A New Perspective
Abstract
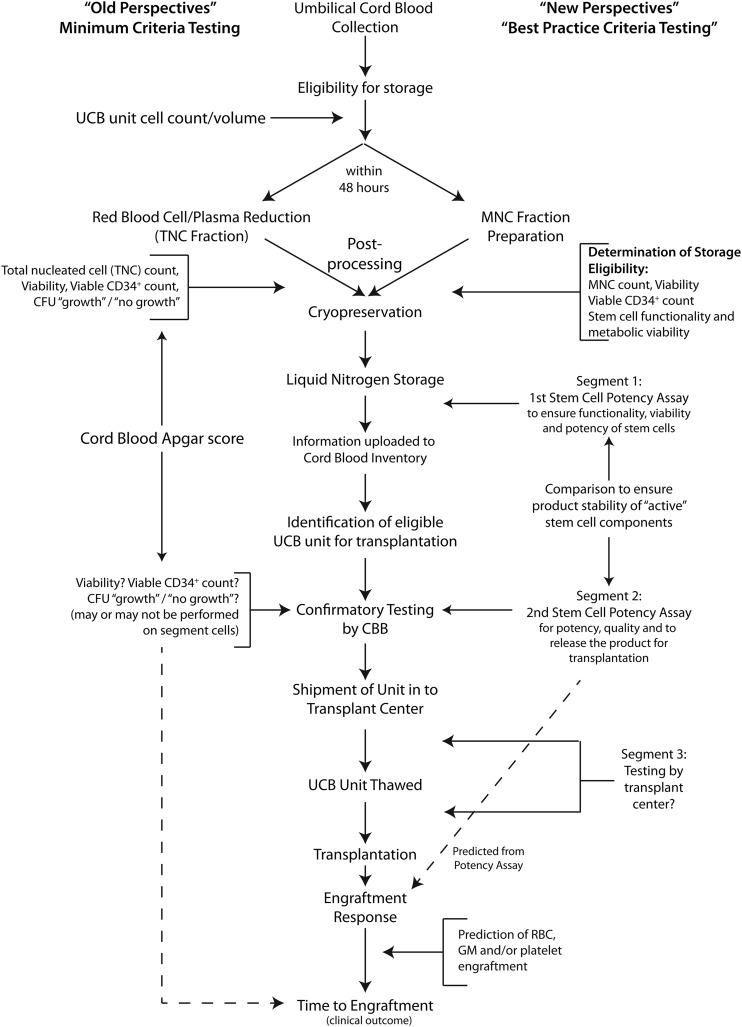
This article critically reviews current methods to test and characterize umbilical cord blood (UCB) for hematopoietic stem cell transplantation. These tests include total nucleated cell (TNC) count, viability, viable CD34-positive content, and the colony-forming unit assay. It is assumed that the data obtained are sufficient to perform a UCB stem cell transplant without actually determining the quality and potency of the stem cells responsible for engraftment. This assumption has led not only to a high graft failure rate attributed to low or lack of potency, but also to noncompliance with present statutes that require UCB stem cells to be of high quality and, indeed, potency for a transplant to be successful. New evidence now calls into question the quality of the data, based on the UCB processed TNC fraction because using this impure fraction masks and significantly underestimates the functionality of the stem cells in both the segment and the unit. It is proposed that UCB units should be processed to the mononuclear cell fraction and that new cost-effective technology that measures the quality and potency of UCB stem cells be implemented to achieve better practices in UCB testing. These changes would provide the transplant physician with the assurance that the stem cells will perform as intended and would reduce risk and increase safety and efficacy for the patient.
Significance: Current stem cell transplantation of umbilical cord blood cells requires testing that includes four basic parameters that do not determine whether the stem cells are of high quality, as required by the Stem Cell Therapeutic and Research Act of 2005. No cord blood units collected or transplanted so far have been tested for stem cell quality or potency. New scientific evidence calls into question cord blood processing and testing practices required by regulatory agencies and standards organizations. A new perspective is described that includes stem cell quality and potency testing that could reduce graft failure rates.
©AlphaMed Press.
Figures
References
-
- Buckner CD, Clift RA, Fefer A, et al. Human marrow transplantation--current status. Prog Hematol. 1973;8:299–324. - PubMed
-
- Haas R, Ho AD, Bredthauer U, et al. Successful autologous transplantation of blood stem cells mobilized with recombinant human granulocyte-macrophage colony-stimulating factor. Exp Hematol. 1990;18:94–98. - PubMed
-
- Körbling M, Holle R, Haas R, et al. Autologous blood stem-cell transplantation in patients with advanced Hodgkin’s disease and prior radiation to the pelvic site. J Clin Oncol. 1990;8:978–985. - PubMed
-
- Gluckman E, Broxmeyer HA, Auerbach AD, et al. Hematopoietic reconstitution in a patient with Fanconi’s anemia by means of umbilical-cord blood from an HLA-identical sibling. N Engl J Med. 1989;321:1174–1178. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
