

Phenotype of asthma-chronic obstructive pulmonary disease overlap syndrome
- PMID: 26161009
- PMCID: PMC4497330
- DOI: 10.3904/kjim.2015.30.4.443
Phenotype of asthma-chronic obstructive pulmonary disease overlap syndrome
Abstract
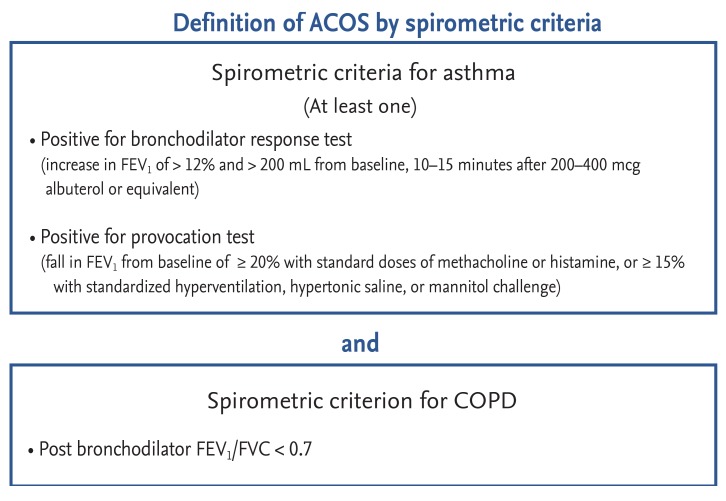
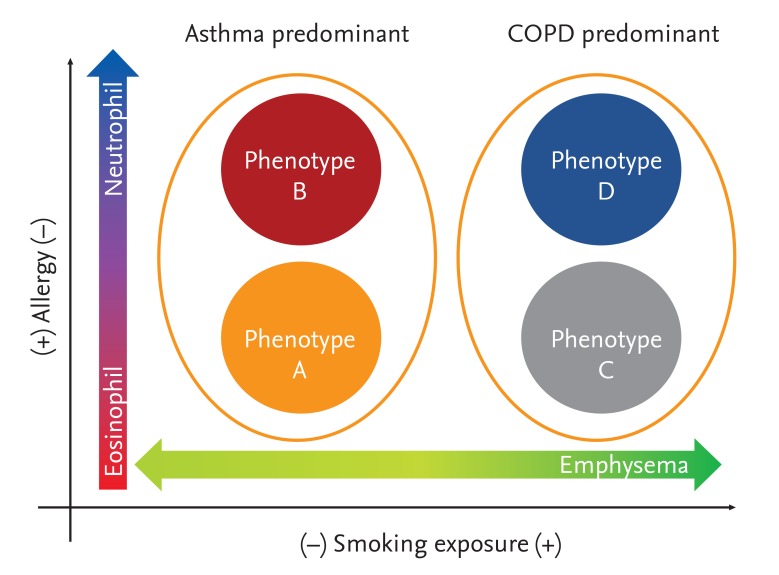
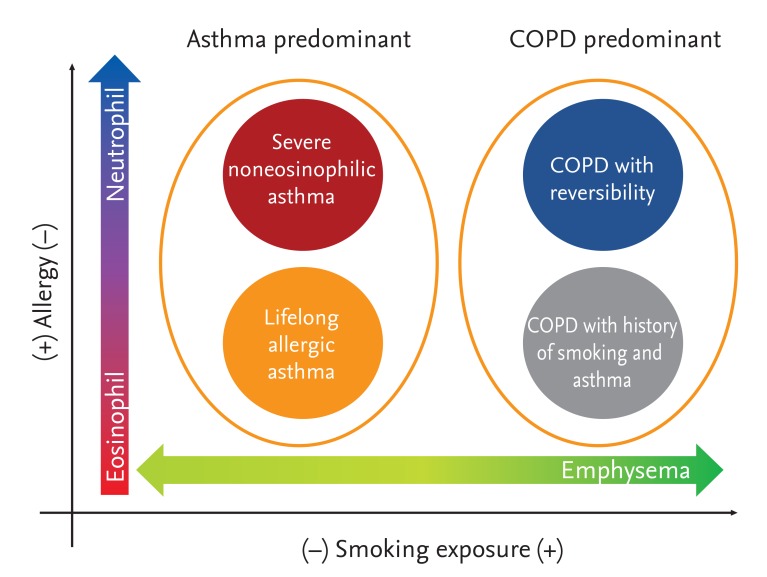
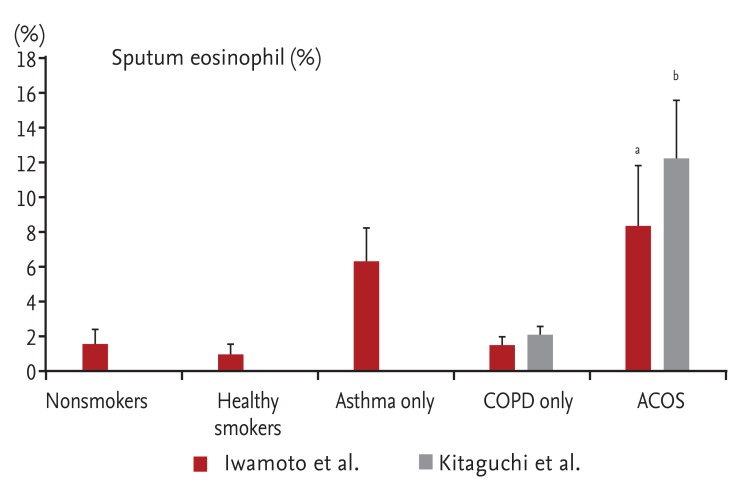
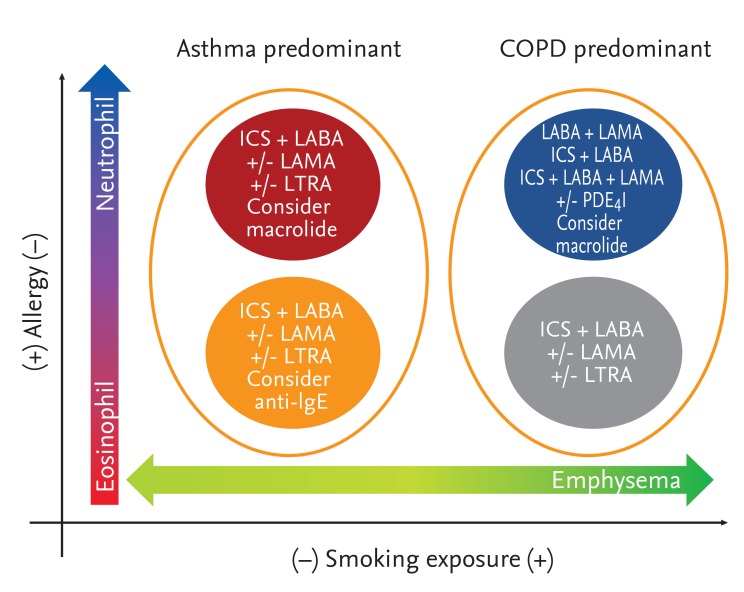
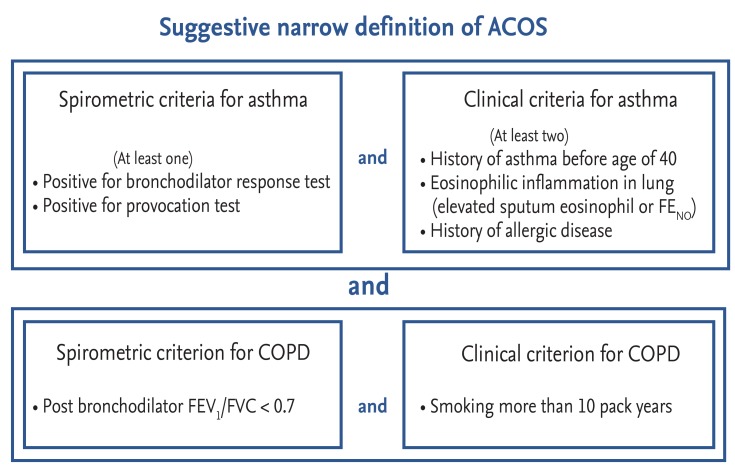
Many patients with asthma or chronic obstructive pulmonary disease (COPD) have overlapping characteristics of both diseases. By spirometric definition, patients with both fixed airflow obstruction (AO) and bronchodilator reversibility or fixed AO and bronchial hyperresponsiveness can be considered to have asthma-COPD overlap syndrome (ACOS). However, patients regarded to have ACOS by spirometric criteria alone are heterogeneous and can be classified by phenotype. Eosinophilic inflammation, a history of allergic disease, and smoke exposure are important components in the classification of ACOS. Each phenotype has a different underlying pathophysiology, set of characteristics, and prognosis. Medical treatment for ACOS should be tailored according to phenotype. A narrower definition of ACOS that includes both spirometric and clinical criteria is needed.
Keywords: Asthma; Phenotype; Pulmonary disease, chronic obstructive.
Conflict of interest statement
Figures
Similar articles
-
The objective evaluation of obstructive pulmonary diseases with spirometry.Int J Chron Obstruct Pulmon Dis. 2016 Aug 25;11:2009-15. doi: 10.2147/COPD.S113774. eCollection 2016. Int J Chron Obstruct Pulmon Dis. 2016. PMID: 27616884 Free PMC article.
-
Clinical, physiological, and radiological features of asthma-chronic obstructive pulmonary disease overlap syndrome.Int J Chron Obstruct Pulmon Dis. 2015 May 15;10:947-54. doi: 10.2147/COPD.S80022. eCollection 2015. Int J Chron Obstruct Pulmon Dis. 2015. PMID: 26028967 Free PMC article.
-
The challenge of diagnosing a mixed asthma-COPD phenotype (ACOS) in clinical practice.Ther Adv Respir Dis. 2016 Apr;10(2):175-8. doi: 10.1177/1753465816630209. Ther Adv Respir Dis. 2016. PMID: 26968234 Free PMC article. No abstract available.
-
[Asthma-COPD overlap syndrome (ACOS)].Nihon Rinsho. 2016 May;74(5):778-82. Nihon Rinsho. 2016. PMID: 27254946 Review. Japanese.
-
Asthma and chronic obstructive pulmonary disease overlap: asthmatic chronic obstructive pulmonary disease or chronic obstructive asthma?Ther Adv Respir Dis. 2016 Feb;10(1):57-71. doi: 10.1177/1753465815617082. Epub 2015 Nov 22. Ther Adv Respir Dis. 2016. PMID: 26596632 Free PMC article. Review.
Cited by
-
A Multifaceted Exploration of Status Asthmaticus: A Retrospective Analysis in a Romanian Hospital.J Clin Med. 2024 Nov 4;13(21):6615. doi: 10.3390/jcm13216615. J Clin Med. 2024. PMID: 39518753 Free PMC article.
-
Toward Precision Medicine in Asthma-Chronic Obstructive Pulmonary Disease Overlap.Allergy Asthma Immunol Res. 2024 Nov;16(6):563-566. doi: 10.4168/aair.2024.16.6.563. Allergy Asthma Immunol Res. 2024. PMID: 39622681 Free PMC article. No abstract available.
-
A comparison of diagnostic consistency for asthma-chronic obstructive pulmonary disease overlap and clinical characteristics study.BMC Pulm Med. 2019 Dec 18;19(1):249. doi: 10.1186/s12890-019-1024-2. BMC Pulm Med. 2019. PMID: 31852476 Free PMC article.
-
Heterogeneity of asthma-COPD overlap syndrome.Int J Chron Obstruct Pulmon Dis. 2017 Feb 22;12:697-703. doi: 10.2147/COPD.S130943. eCollection 2017. Int J Chron Obstruct Pulmon Dis. 2017. PMID: 28260876 Free PMC article.
-
Glucocorticoid Use in Patients Hospitalized with Chronic Obstructive Pulmonary Disease Exacerbations.Int J Chron Obstruct Pulmon Dis. 2024 Feb 12;19:431-438. doi: 10.2147/COPD.S436326. eCollection 2024. Int J Chron Obstruct Pulmon Dis. 2024. PMID: 38371231 Free PMC article.
References
-
- Gibson PG, Simpson JL. The overlap syndrome of asthma and COPD: what are its features and how important is it. Thorax. 2009;64:728–735. - PubMed
-
- Lange P, Parner J, Vestbo J, Schnohr P, Jensen G. A 15-year follow-up study of ventilatory function in adults with asthma. N Engl J Med. 1998;339:1194–1200. - PubMed
-
- James AL, Palmer LJ, Kicic E, et al. Decline in lung function in the Busselton Health Study: the effects of asthma and cigarette smoking. Am J Respir Crit Care Med. 2005;171:109–114. - PubMed
-
- Thomsen M, Nordestgaard BG, Vestbo J, Lange P. Characteristics and outcomes of chronic obstructive pulmonary disease in never smokers in Denmark: a prospective population study. Lancet Respir Med. 2013;1:543–550. - PubMed
-
- Ulrik CS, Backer V. Nonreversible airflow obstruction in life-long nonsmokers with moderate to severe asthma. Eur Respir J. 1999;14:892–896. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical