

Review
doi: 10.3978/j.issn.2227-684X.2015.04.22.
Current strategies with 2-staged prosthetic breast reconstruction
Affiliations
- PMID: 26161305
- PMCID: PMC4461711
- DOI: 10.3978/j.issn.2227-684X.2015.04.22
Item in Clipboard
Review
Current strategies with 2-staged prosthetic breast reconstruction
Gland Surg.
2015 Jun.
Abstract
Over the last decade, prosthetic-based breast reconstruction has been revolutionized with technological advancements. Reconstructive surgeons now have a multitude of prosthetic devices and tissue expanders, tools for intraoperative perfusion analysis, implantable bioprosthetic materials and a technique for autoaugmentation within their armamentarium to reconstruct natural breasts today like never before.
Keywords: Breast reconstruction; acellular dermal matrix (ADM); breast implants; fat grafting; implant-based breast reconstruction; laser-assisted indocyanine green angiography; prosthetic-based breast reconstruction.
Figures
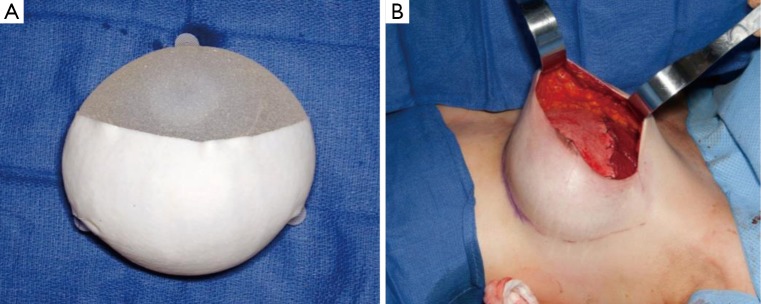
(A) Standard tissue expander device with partial ADM coverage. Note textured surface, tabs and incorporation of filling port. (B) In a standard 2-staged reconstruction, this device is placed in the subpectoral plane with the superior aspect being covered with the pectoralis major.
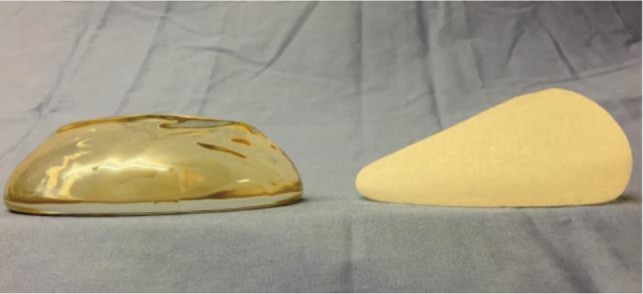
Silicone breast implants. A round, smooth-textured implant on the left. A textured, anatomic implant on the right.
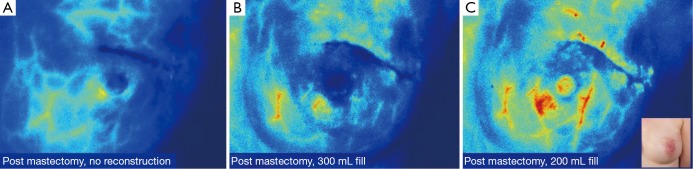
(A) Prior to beginning the reconstruction, post-mastectomy intraoperative LA-ICGA revealed adequate perfusion to the nipple-areolar complex; (B) 550 mL tissue expanders filled to 300 mL, were placed in the partial subpectoral pocket with the lower pole reinforced with ADM. Repeat LA-ICGA showed compromised perfusion to the left upper outer quadrant; (C) the left tissue expander was partially deflated and repeat LA-ICGA revealed adequate perfusion. LA-ICGA, laser-assisted indocyanine green fluorescent angiography; ADM, acellular dermal matrix.
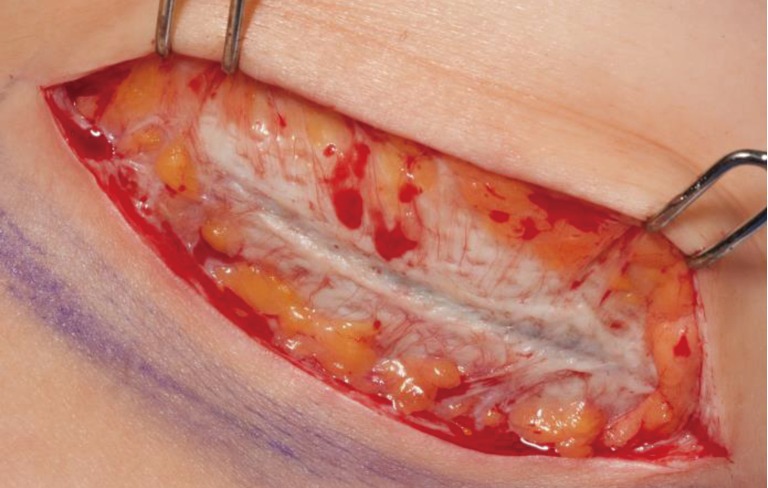
Incorporated ADM showing revascularization at time of second stage from tissue expander to implant (3 months). ADM, acellular dermal matrix.
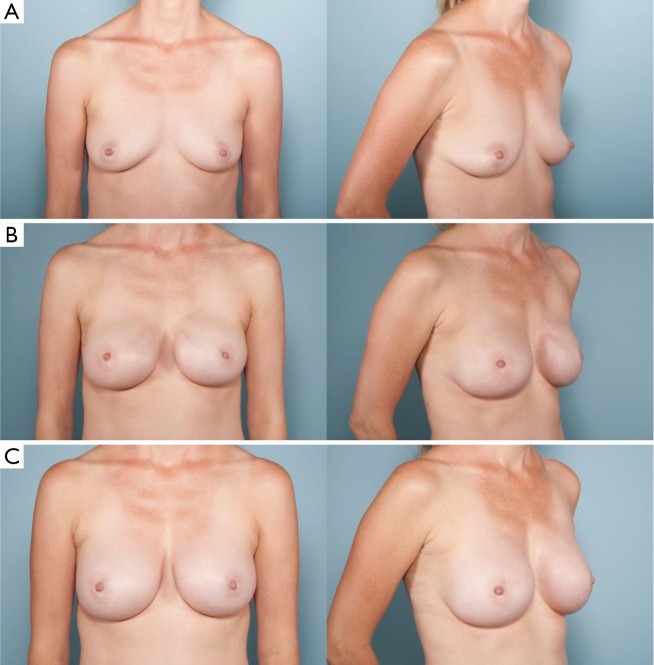
(A) Preoperative photographs of a patient with right breast cancer; (B) after undergoing bilateral nipple-sparing mastectomies with immediate tissue expander placement in the subcutaneous plane through an inframammary fold approach; (C) final reconstruction after exchange of tissue expander for anatomic silicone breast implants and fat grafting.
References
-
- U.S. Breast Cancer Statistics. September 20, 2014. Available online: http://www.breastcancer.org/symptoms/understand_bc/statistics
-
- Surgeons ASoP. 2014 Reconstructive Plastic Surgery Statistics. 2014.
-
- Ng SK, Hare RM, Kuang RJ, et al. Breast Reconstruction Post Mastectomy: Patient Satisfaction and Decision Making. Ann Plast Surg 2014. [Epub ahead of print]. - PubMed
-
- Serletti JM, Fosnot J, Nelson JA, et al. Breast reconstruction after breast cancer. Plast Reconstr Surg 2011;127:124e-35e. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical