

New Algorithm for Managing Childhood Illness Using Mobile Technology (ALMANACH): A Controlled Non-Inferiority Study on Clinical Outcome and Antibiotic Use in Tanzania
- PMID: 26161535
- PMCID: PMC4498627
- DOI: 10.1371/journal.pone.0132316
New Algorithm for Managing Childhood Illness Using Mobile Technology (ALMANACH): A Controlled Non-Inferiority Study on Clinical Outcome and Antibiotic Use in Tanzania
Abstract
Introduction: The decline of malaria and scale-up of rapid diagnostic tests calls for a revision of IMCI. A new algorithm (ALMANACH) running on mobile technology was developed based on the latest evidence. The objective was to ensure that ALMANACH was safe, while keeping a low rate of antibiotic prescription.
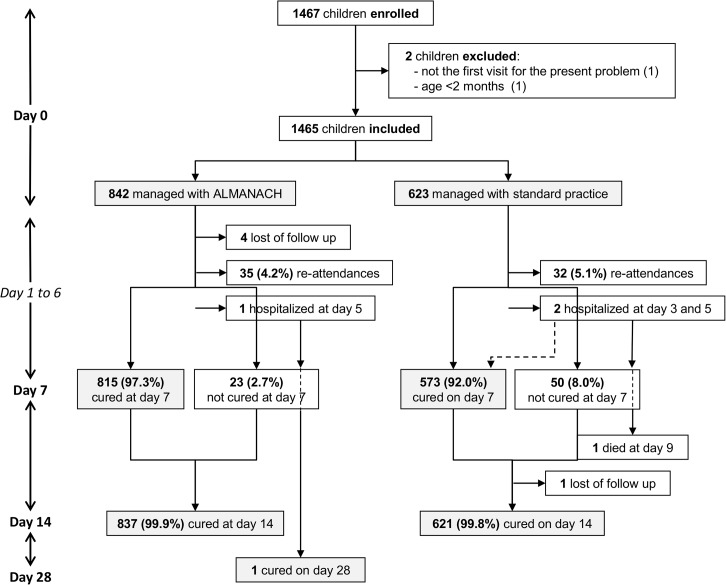
Methods: Consecutive children aged 2-59 months with acute illness were managed using ALMANACH (2 intervention facilities), or standard practice (2 control facilities) in Tanzania. Primary outcomes were proportion of children cured at day 7 and who received antibiotics on day 0.
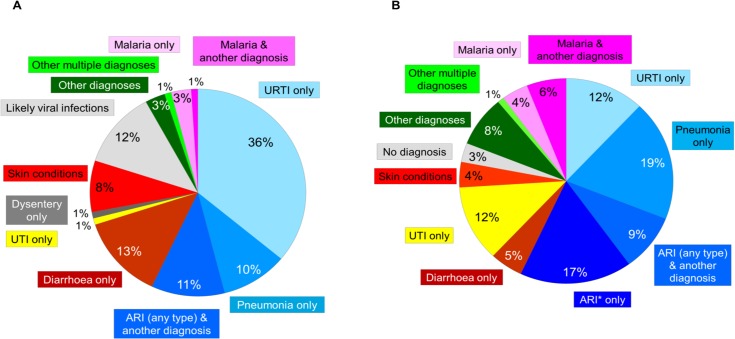
Results: 130/842 (15∙4%) in ALMANACH and 241/623 (38∙7%) in control arm were diagnosed with an infection in need for antibiotic, while 3∙8% and 9∙6% had malaria. 815/838 (97∙3%;96∙1-98.4%) were cured at D7 using ALMANACH versus 573/623 (92∙0%;89∙8-94∙1%) using standard practice (p<0∙001). Of 23 children not cured at D7 using ALMANACH, 44% had skin problems, 30% pneumonia, 26% upper respiratory infection and 13% likely viral infection at D0. Secondary hospitalization occurred for one child using ALMANACH and one who eventually died using standard practice. At D0, antibiotics were prescribed to 15∙4% (12∙9-17∙9%) using ALMANACH versus 84∙3% (81∙4-87∙1%) using standard practice (p<0∙001). 2∙3% (1∙3-3.3) versus 3∙2% (1∙8-4∙6%) received an antibiotic secondarily.
Conclusion: Management of children using ALMANACH improve clinical outcome and reduce antibiotic prescription by 80%. This was achieved through more accurate diagnoses and hence better identification of children in need of antibiotic treatment or not. The building on mobile technology allows easy access and rapid update of the decision chart.
Trial registration: Pan African Clinical Trials Registry PACTR201011000262218.
Conflict of interest statement
Figures
References
-
- Claeson M, Gillespie D, Mshinda H, Troedsson H, Victora CG. Knowledge into action for child survival. Lancet. 2003;362(9380):323–7. - PubMed
-
- Armstrong Schellenberg JR, Adam T, Mshinda H, Masanja H, Kabadi G, Mukasa O, et al. Effectiveness and cost of facility-based Integrated Management of Childhood Illness (IMCI) in Tanzania. Lancet. 2004;364(9445):1583–94. Epub 2004/11/03. doi: S014067360417311X [pii] 10.1016/S0140-6736(04)17311-X . - DOI - PubMed
-
- Gouws E, Bryce J, Habicht JP, Amaral J, Pariyo G, Schellenberg JA, et al. Improving antimicrobial use among health workers in first-level facilities: results from the multi-country evaluation of the Integrated Management of Childhood Illness strategy. Bull World Health Organ. 2004;82(7):509–15. Epub 2004/10/29. . - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
