

Accounting for False Positive HIV Tests: Is Visceral Leishmaniasis Responsible?
- PMID: 26161864
- PMCID: PMC4498794
- DOI: 10.1371/journal.pone.0132422
Accounting for False Positive HIV Tests: Is Visceral Leishmaniasis Responsible?
Abstract
Background: Co-infection with HIV and visceral leishmaniasis is an important consideration in treatment of either disease in endemic areas. Diagnosis of HIV in resource-limited settings relies on rapid diagnostic tests used together in an algorithm. A limitation of the HIV diagnostic algorithm is that it is vulnerable to falsely positive reactions due to cross reactivity. It has been postulated that visceral leishmaniasis (VL) infection can increase this risk of false positive HIV results. This cross sectional study compared the risk of false positive HIV results in VL patients with non-VL individuals.
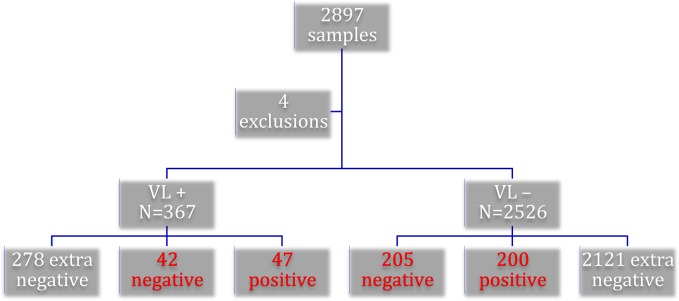
Methodology/principal findings: Participants were recruited from 2 sites in Ethiopia. The Ethiopian algorithm of a tiebreaker using 3 rapid diagnostic tests (RDTs) was used to test for HIV. The gold standard test was the Western Blot, with indeterminate results resolved by PCR testing. Every RDT screen positive individual was included for testing with the gold standard along with 10% of all negatives. The final analysis included 89 VL and 405 non-VL patients. HIV prevalence was found to be 12.8% (47/ 367) in the VL group compared to 7.9% (200/2526) in the non-VL group. The RDT algorithm in the VL group yielded 47 positives, 4 false positives, and 38 negatives. The same algorithm for those without VL had 200 positives, 14 false positives, and 191 negatives. Specificity and positive predictive value for the group with VL was less than the non-VL group; however, the difference was not found to be significant (p = 0.52 and p = 0.76, respectively).
Conclusion: The test algorithm yielded a high number of HIV false positive results. However, we were unable to demonstrate a significant difference between groups with and without VL disease. This suggests that the presence of endemic visceral leishmaniasis alone cannot account for the high number of false positive HIV results in our study.
Conflict of interest statement
Figures
References
-
- World Health Organization (2012) Service delivery approaches to HIV testing and Counselling (HTC) Geneva, WHO.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
