

Olfactomedin 4 Serves as a Marker for Disease Severity in Pediatric Respiratory Syncytial Virus (RSV) Infection
- PMID: 26162090
- PMCID: PMC4498630
- DOI: 10.1371/journal.pone.0131927
Olfactomedin 4 Serves as a Marker for Disease Severity in Pediatric Respiratory Syncytial Virus (RSV) Infection
Abstract
Background: Respiratory viral infections follow an unpredictable clinical course in young children ranging from a common cold to respiratory failure. The transition from mild to severe disease occurs rapidly and is difficult to predict. The pathophysiology underlying disease severity has remained elusive. There is an urgent need to better understand the immune response in this disease to come up with biomarkers that may aid clinical decision making.
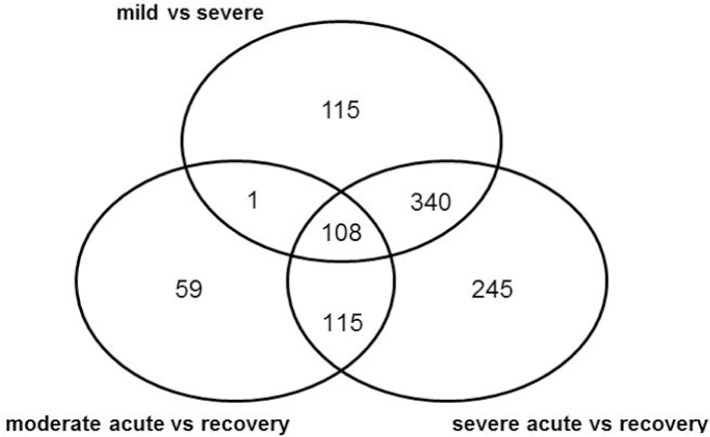
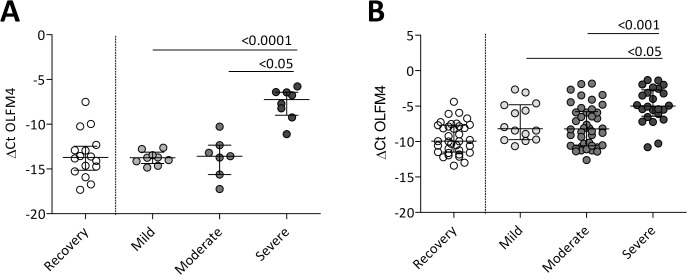
Methods: In a prospective study, flow cytometric and genome-wide gene expression analyses were performed on blood samples of 26 children with a diagnosis of severe, moderate or mild Respiratory Syncytial Virus (RSV) infection. Differentially expressed genes were validated using Q-PCR in a second cohort of 80 children during three consecutive winter seasons. FACS analyses were also performed in the second cohort and on recovery samples of severe cases in the first cohort.
Results: Severe RSV infection was associated with a transient but marked decrease in CD4+ T, CD8+ T, and NK cells in peripheral blood. Gene expression analyses in both cohorts identified Olfactomedin4 (OLFM4) as a fully discriminative marker between children with mild and severe RSV infection, giving a PAM cross-validation error of 0%. Patients with an OLFM4 gene expression level above -7.5 were 6 times more likely to develop severe disease, after correction for age at hospitalization and gestational age.
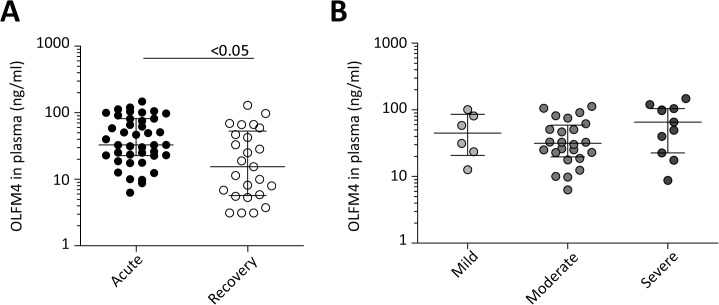
Conclusion: By combining genome-wide expression profiling of blood cell subsets with clinically well-annotated samples, OLFM4 was identified as a biomarker for severity of pediatric RSV infection.
Conflict of interest statement
Figures
References
-
- Henrickson KJ, Hoover S, Kehl KS, Hua W. National disease burden of respiratory viruses detected in children by polymerase chain reaction. Pediatr Infect Dis J. 2004;23(1 Suppl):S11–8. - PubMed
-
- Iwane MK, Edwards KM, Szilagyi PG, Walker FJ, Griffin MR, Weinberg GA, et al. Population-based surveillance for hospitalizations associated with respiratory syncytial virus, influenza virus, and parainfluenza viruses among young children. Pediatrics. 2004;113(6):1758–64. - PubMed
-
- Shay DK, Holman RC, Newman RD, Liu LL, Stout JW, Anderson LJ. Bronchiolitis-associated hospitalizations among US children, 1980–1996. JAMA: the journal of the American Medical Association. 1999;282(15):1440–6. - PubMed
-
- Black CP. Systematic review of the biology and medical management of respiratory syncytial virus infection. Respiratory care. 2003;48(3):209–31; discussion 31–3. - PubMed
-
- Boyce TG, Mellen BG, Mitchel EF Jr., Wright PF, Griffin MR. Rates of hospitalization for respiratory syncytial virus infection among children in medicaid. J Pediatr. 2000;137(6):865–70. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
