

Rewarming Rate During Cardiopulmonary Bypass Is Associated With Release of Glial Fibrillary Acidic Protein
- PMID: 26163357
- PMCID: PMC4593711
- DOI: 10.1016/j.athoracsur.2015.04.006
Rewarming Rate During Cardiopulmonary Bypass Is Associated With Release of Glial Fibrillary Acidic Protein
Abstract
Background: Rewarming from hypothermia during cardiopulmonary bypass (CPB) may compromise cerebral oxygen balance, potentially resulting in cerebral ischemia. The purpose of this study was to evaluate whether CPB rewarming rate is associated with cerebral ischemia assessed by the release of the brain injury biomarker glial fibrillary acidic protein (GFAP).
Methods: Blood samples were collected from 152 patients after anesthesia induction and after CPB for the measurement of plasma GFAP levels. Nasal temperatures were recorded every 15 min. A multivariate estimation model for postoperative plasma GFAP level was determined that included the baseline GFAP levels, rewarming rate, CPB duration, and patient age.
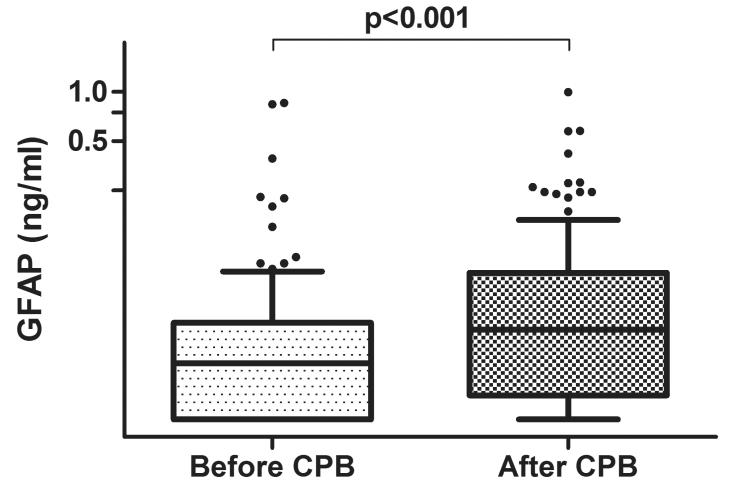
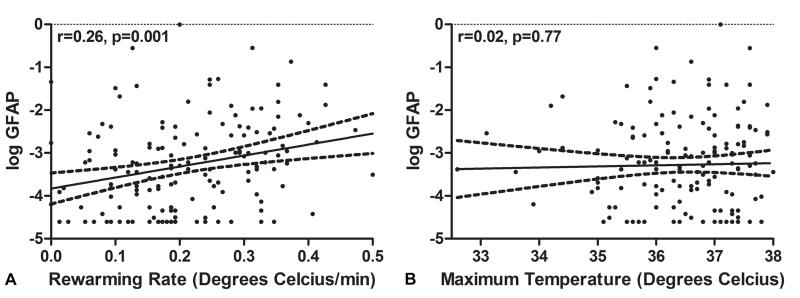
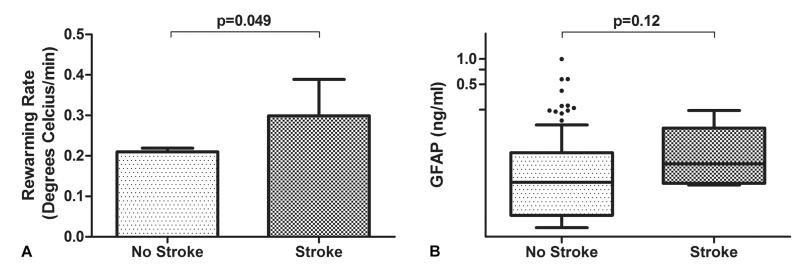
Results: The mean rewarming rate during CPB was 0.21° ± 0.11°C/min; the maximal temperature was 36.5° ± 1.0°C (range, 33.1°C to 38.0°C). Plasma GFAP levels increased after compared with before CPB (median, 0.022 ng/mL versus 0.035 ng/mL; p < 0.001). Rewarming rate (p = 0.001), but not maximal temperature (p = 0.77), was associated with higher plasma GFAP levels after CPB. In the adjusted estimation model, rewarming rate was positively associated with postoperative plasma log GFAP levels (coefficient, 0.261; 95% confidence intervals, 0.132 to 0.390; p < 0.001). Six patients (3.9%) experienced a postoperative stroke. Rewarming rate was higher (0.3° ± 0.09°C/min versus 0.2° ± 0.11°C/min; p = 0.049) in the patients with stroke compared with those without a stroke.
Conclusions: Rewarming rate during CPB was correlated with evidence of brain cellular injury documented with plasma GFAP levels. Modifying current practices of patient rewarming might provide a strategy to reduce the frequency of neurologic complications after cardiac surgery.
Copyright © 2015 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Invited Commentary.Ann Thorac Surg. 2015 Oct;100(4):1358-9. doi: 10.1016/j.athoracsur.2015.05.004. Ann Thorac Surg. 2015. PMID: 26434434 No abstract available.
-
Rapid Rewarming During Cardiopulmonary Bypass Is Associated With Cerebral Injury.Ann Thorac Surg. 2016 May;101(5):2026-7. doi: 10.1016/j.athoracsur.2015.11.021. Ann Thorac Surg. 2016. PMID: 27106452 No abstract available.
-
Reply.Ann Thorac Surg. 2016 May;101(5):2027. doi: 10.1016/j.athoracsur.2015.11.053. Ann Thorac Surg. 2016. PMID: 27106453 No abstract available.
Similar articles
-
Cardiopulmonary Bypass Increases Plasma Glial Fibrillary Acidic Protein Only in First Stage Palliation of Hypoplastic Left Heart Syndrome.Can J Cardiol. 2016 Mar;32(3):355-61. doi: 10.1016/j.cjca.2015.06.023. Epub 2015 Jul 2. Can J Cardiol. 2016. PMID: 26481085
-
Glial fibrillary acidic protein plasma levels are correlated with degree of hypothermia during cardiopulmonary bypass in congenital heart disease surgery.Interact Cardiovasc Thorac Surg. 2017 Mar 1;24(3):436-442. doi: 10.1093/icvts/ivw395. Interact Cardiovasc Thorac Surg. 2017. PMID: 28040762
-
Cardiopulmonary-Bypass Glial Fibrillary Acidic Protein Correlates With Neurocognitive Skills.Ann Thorac Surg. 2018 Sep;106(3):792-798. doi: 10.1016/j.athoracsur.2018.03.083. Epub 2018 May 5. Ann Thorac Surg. 2018. PMID: 29733822
-
The Society of Thoracic Surgeons, The Society of Cardiovascular Anesthesiologists, and The American Society of ExtraCorporeal Technology: Clinical Practice Guidelines for Cardiopulmonary Bypass--Temperature Management During Cardiopulmonary Bypass.J Cardiothorac Vasc Anesth. 2015 Aug;29(4):1104-13. doi: 10.1053/j.jvca.2015.07.011. J Cardiothorac Vasc Anesth. 2015. PMID: 26279227 Review.
-
The neurologic sequelae of cardiopulmonary bypass-induced cerebral hyperthermia and cerebroprotective strategies.J Extra Corpor Technol. 2003 Dec;35(4):317-21. J Extra Corpor Technol. 2003. PMID: 14979423 Review.
Cited by
-
Frailty, Aging, and Cardiovascular Surgery.Anesth Analg. 2017 Apr;124(4):1053-1060. doi: 10.1213/ANE.0000000000001560. Anesth Analg. 2017. PMID: 27622718 Free PMC article. Review.
-
Changes in Plasma Glial Fibrillary Acidic Protein in Children Receiving Sevoflurane Anesthesia: A Preliminary Randomized Trial.J Clin Med. 2021 Feb 9;10(4):662. doi: 10.3390/jcm10040662. J Clin Med. 2021. PMID: 33572213 Free PMC article.
-
Recent innovations in perfusion and cardiopulmonary bypass for neonatal and infant cardiac surgery.Transl Pediatr. 2018 Apr;7(2):139-150. doi: 10.21037/tp.2018.03.05. Transl Pediatr. 2018. PMID: 29770295 Free PMC article. Review.
-
A pilot goal-directed perfusion initiative is associated with less acute kidney injury after cardiac surgery.J Thorac Cardiovasc Surg. 2017 Jan;153(1):118-125.e1. doi: 10.1016/j.jtcvs.2016.09.016. Epub 2016 Sep 19. J Thorac Cardiovasc Surg. 2017. PMID: 27832832 Free PMC article.
-
Biomarkers improve prediction of 30-day unplanned readmission or mortality after paediatric congenital heart surgery.Cardiol Young. 2019 Aug;29(8):1051-1056. doi: 10.1017/S1047951119001471. Epub 2019 Jul 10. Cardiol Young. 2019. PMID: 31290383 Free PMC article.
References
-
- Busto R, Globus MY, Dietrich WD, Martinez E, Valdes I, Ginsberg MD. Effect of mild hypothermia on ischemia-induced release of neurotransmitters and free fatty acids in rat brain. Stroke. 1989;20(7):904–10. - PubMed
-
- Kil HY, Zhang J, Piantadosi CA. Brain temperature alters hydroxyl radical production during cerebral ischemia/reperfusion in rats. J Cereb Blood Flow Metab. 1996;16(1):100–6. - PubMed
-
- White BC, Sullivan JM, DeGracia DJ, et al. Brain ischemia and reperfusion: molecular mechanisms of neuronal injury. J Neurol Sci. 2000;179(S1-2):1–33. - PubMed
-
- Winfree CJ, Baker CJ, Connolly ES, Jr, Fiore AJ, Solomon RA. Mild hypothermia reduces penumbral glutamate levels in the rat permanent focal cerebral ischemia model. Neurosurgery. 1996;38(6):1216–22. - PubMed
-
- Castillo J, Davalos A, Noya M. Aggravation of acute ischemic stroke by hyperthermia is related to an excitotoxic mechanism. Cerebrovasc Dis. 1999;9(1):22–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
